This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
Neurologic deficits, seizures, cognitive issues, hearing loss. Give acyclovir If there is concern for HSV encephalitis (focal neurologic deficits, seizures, markedly depressed mental status, or immunocompromise) The mortality rate for HSV encephalitis is up to 70%. Mortality rate is 10-30%. HSV meningitis needs hospital admission.
There is substantial evidence that IV fluids can be beneficial in patients with sepsis complicated by hypotension and labor. Patients receiving maintenance fluids are hemodynamically stable, but they are unable to orally meet their daily fluid and electrolyte requirements.
We cover leadership through change, IN midazolam for pediatric seizure, hypothermia and young infant sepsis risk, VICTAS RCT, and clinically diagnosing GHB intoxication. It’s the JournalFeed Podcast for the week of Apr 19-23, 2021.
35-year-old man presents by EMS with seizures. According to family at the scene, he has a history of seizures but has not been taking his medication recently. On arrival, he is obtunded, foaming at the mouth, and exhibiting generalized tonic-clonic seizure activity. Clinical Question » How should status epilepticus be diagnosed?
The study was performed when Surviving Sepsis Campaign Guidelines were used, so it was more common to see large volume fluid administration in the setting of sepsis. vs 48.4% (OR 3.4, 5.53) Takeaways: Positive trial => there was a statistically significant rate of shock control attained with the treatment arm. vs 48.4% (OR 3.4,
They have a seizure on arrival and a Na comes back at 105. In this scenario they are seizing because of the low Na and rapid increase of the Na is needed to stop the seizure. A seizure seems fairly easy to define but “coma” is a little bit more vague. They have a seizure on arrival and a Na comes back at 105.
Eclampsia (B) is characterized by the onset of seizures in a woman with preeclampsia (hypertension and proteinuria), but it typically does not present with the sudden onset of respiratory distress and profound hypotension described here. . “Markers of Inflammation and Infection in Sepsis and Disseminated Intravascular Coagulation.”
Unfortunately, it can cause so many other complications – Sepsis , acute chest syndrome , and hepatopathy. If Sickle Cell Disease only ever caused Vaso-Occlusive crises, it would be considered one of the most challenging conditions for patients and families to deal with.
The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. As may be seen in the table below, there are several themes as well a range of stringency. C., & Solomon, T. The Journal of infection , 72 (4), 405–438. van de Beek, D., Cabellos, C.,
Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. Following the triage sepsis pathway, recently amended to use qSOFA.
Capnography has several novel uses in other disease states commonly seen in the ED such as trauma, DKA, sepsis and obstructive lung disease. In cardiac arrest, EtCO 2 is dependent on compressions AND the underlying cause. ETCO 2 correlates with blood pressure, lactate, and base excess in critically ill patients.
Often AE-ILD is idiopathic, but treatable causes must be excluded (PNA, PE, volume overload) Treatment for AE-ILD should include antibiotics for CAP coverage (specifically including azithromycin), steroids, and respiratory support; consider opportunistic infection if immunosuppressed as well as diuresis as needed for euvolemia HFNC should be favored (..)
1 , 2 The most common non-iatrogenic cause is spontaneously due to increased intraesophageal pressure, Boerhaave syndrome, from forceful retching, coughing, straining, seizures, or even childbirth (15% of cases). upper endoscopy, transesophageal echo, etc.). upper endoscopy, transesophageal echo, etc.).
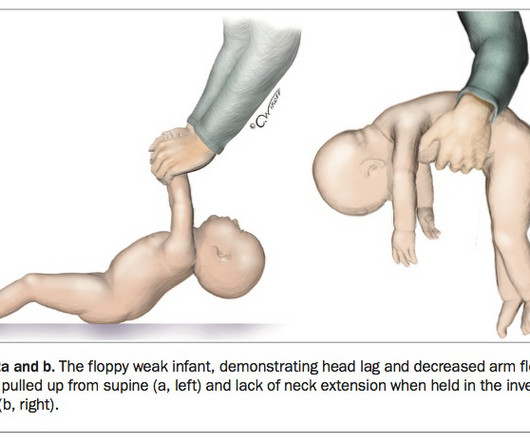
Were there any risk factors for sepsis? Increased work of breathing with grunting and tachypnoea could be due to sepsis, hypoglycaemia or acidosis due to an inborn error of metabolism. Severe jaundice causing kernicterus may also cause central hypotonia and seizures. Birth History How long was the labour?
Definition of status epilepticus:Continuous seizure activity of 5 minutes or greater – OR – Recurrent activity without recovery between intervals. This definition includes clinically apparent seizures as well as those seen only on EEG.) During a seizure, GABA receptors in the neuron’s membrane are internalized and destroyed.
meningoencephalitis, overwhelming alternate source of sepsis) T – Toxins (e.g. sludge phenomenon, secondary sepsis, hypoglycemia from supply-demand mismatch) S – Seizure (e.g. meningoencephalitis, overwhelming alternate source of sepsis) T – Toxins (e.g. V – Vascular (e.g. V – Vascular (e.g. Should you get a CT before LP?
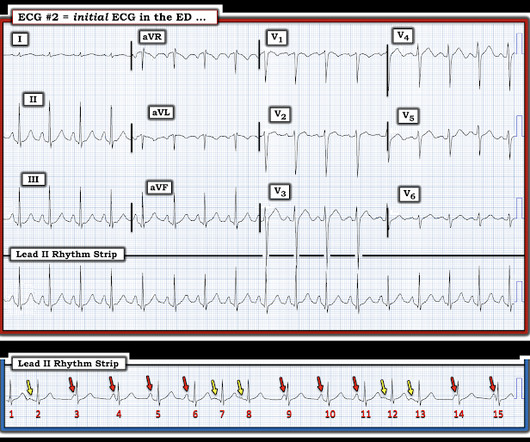
Most occurrences are associated with events such as sepsis, shock, recent infarction, post-operative state, electrolyte disturbance — or "sick patient". Seizure activity was witnessed at the scene — and head CT scan showed a small bleed. PEARL # 5: Accelerated junctional rhythms are not common in adults.
Perhaps diGeorge syndrome with hypocalcemia and seizures? Inborn Errors of Metabolism - there are over 200 inborn errors of metabolism, but only four common metabolic pathways that cause a child to be critically ill. Before you decide on sepsis, ask yourself, could this be a cardiac problem?*
Cefepime crosses the blood-brain barrier, and dozens of case reports have associated the drug with seizures, encephalopathy, delirium, and coma, with a possibly increased incidence of neurologic adverse effects among patients with renal failure or sepsis.
They include neurologic dysfunction, which is one of the most common that includes things like developmental delay, regression, AKA loss of developmental milestones, hypotonia, encephalopathy, or seizures. So they’re lethargic, they might vomit, they’re hypotonic, hypothermic, they might have fever or seizures.
They were worried that the syncope was seizure and that she had brain mets. Then they were worried about sepsis as an etiology of hypotension. Then she had some RUQ tenderness which led to a long process of evaluation for an abdominal source of sepsis, which turned up negative. Previous ECG. The lactate was elevated and pH low.
Lactate A sick child with sepsis syndrome? In the adult literature, we know that a lactate level above 4 mmol/L in patients with severe sepsis was associated with the need for critical care. The acute recognition and treatment of sepsis is first and foremost, clinical. The short answer – yes.
In terms of reasons to sedate someone in the ICU the following would seem a reasonable selection of reasons * as treatment for disease process (eg seizures, alcohol withdrawal) * to facilitate tolerance of ICU therapies (eg ventilation) * to reduce O2 consumption (eg brain injury or sepsis) * use as palliation In terms of assessing sedation I think (..)
Exertional Hyperthermia Patients with heat stroke will present with Temp > 104, AMS, or seizures. EMS was bagging him on arrival Primary notable for Compromised Airway Protection, bilateral Breath sounds, strong pulses,GCS 3 CT images of Head, Chest, Abdomen, Pelvis, and Spine No acute findings pH of 6.75
stent, percutaneous nephrostomy) by urology or IR Hypokalemia evaluate for EKG changes assess for underlying cause and factors that may influence ability to replete (i.e. Vaishnav Hyperthermia: abnormally high body temperature due to thermoregulatory failure Severe hyperthermia: temp greater than 40.5C
Check the bilirubin in any neonate you are working up for sepsis. Acute bilirubin encephalopathy may progress to an abnormal neurologic exam, seizures, apnea, or coma. The dehydration and neurologic dysfnction from the hyperbilirubinemia may even cause fever. Kernicterus is the final, permanent result of bilirubin encephalpathy.
These require swabs, antibiotics, potentially a sepsis screen and bleeping your registrar / consultant for further advice. encephalopathy, pericarditis, seizures) *common dialysable toxins include lithium, aspirin, theophylline along with many others. Peritoneal dialysis has a risk of infection (PD peritonitis or exit site infection).
8 Workup and Diagnosis Evaluation should be tailored to the patient presentation, but may include studies such as: CBC, CMP, UA, lactate (if concern for sepsis), Cultures (blood, urine, etc.) Imipenem confers highest risk of seizures ESBL-E are often hospital acquired infections and can prolong hospital stay or lead to worse outcomes.
Signs and symptoms in this group are often non-specific and can include irritability, hypotonia, lethargy, jitteriness, temperature instability, poor feeding, vomiting, apnoea and seizures. What’s all this fuss about ketones? All of the cases so far have featured ketotic hypoglycaemia.
Because of this possible diagnosis, they were commenced on a macrolide antibiotic (azithromycin) in addition to treatment for neonatal sepsis +/- meningitis (ceftriaxone and acyclovir). Infants usually present in a non-specific manner, following an apnoea, cough, cyanosis, or seizure so a high index of suspicion is required in this age group.
HAJDU Mild TBI’s & Concussions in the Emergency Department TBI’s are relatively common >3 million TBI’s in the US annually 2.5 million presentation to ED’s throughout the US Usually occur due to falls Also commonly occur due to sports, MVC’s, etc.
Vaccination: PCV13 (pneumococcal vaccination), meningococcal vaccines, and Hib conjugated vaccines are important to prevent life-threatening sepsis. Sickle cell patients also qualify to receive the annual influenza vaccine, since influenza virus infection predisposes to bacterial pneumonia and sepsis caused by S. Pneumococcal sepsis B.
haffner and wright The number of psychiatric emergencies across the U.S., haffner and wright The number of psychiatric emergencies across the U.S., mg/kg (of 0.1 mg/kg (of 0.1 2x maintenance rate
These can lead to a wide spectrum of emergent complications including but not limited to cardiac dysrhythmias, seizures, and acute renal failure. This can often become significant enough to precipitate dysrhythmias, seizures, and tetany (20). paclitaxel, doxorubicin, cisplatin) high-risk monoclonal antibody treatments (i.e.
Cefepime crosses the blood-brain barrier, and dozens of case reports have associated the drug with seizures, encephalopathy, delirium, and coma, with a possibly increased incidence of neurologic adverse effects among patients with renal failure or sepsis.
Clinical recommendations for pain, sedation, withdrawal, and delirium assessment in critically ill infants and children Pediatric Acute Lung Injury and Sepsis Investigators ( PALISI ). Examples of these are linked below: European Society of Paediatric and Neonatal Intensive Care ( ESPNIC ). Am J Respir Crit Care Med. 2023;207(1):17-28.
Complications include death, scarring, skin superinfection, sepsis, encephalitis, meningitis, febrile seizures, and premature birth. The lesions are 7-10 mm in diameter, round, firm, deep-seated and well circumscribed… ” Lesions tend to appear more on the forearms and face than rest of the body.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content