This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Shunting of blood to the extremities results in thermal dysregulation and subsequent hypothermia. Orenstein JB, Klein BL, Gotschall CS, Ochsenschlager DW, Klatzko MD, Eichelberger MR. Age and outcome in pediatric cervical spine injury: 11-year experience. Unopposed vagal tone leads to bradycardia. J Pediatr Surg. 2001;36(2):373.
You are tidying your things […] The post SGEM#391: Is it Time for a Cool Change (Hypothermia After In-Hospital Cardiac Arrest)? Are we supposed to be starting hypothermia?” The hypothermia group was cooled using an external device to a target temperature between 32 and 34 degrees Celsius and maintained there for 24 hours.
Case: A 59-year-old […] The post SGEM#275: 10th Avenue Freeze Out – Therapeutic Hypothermia after Non-Shockable Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Background: We have covered therapeutic hypothermia many times on the SGEM. Date: November 6th, 2019 Reference: Lascarrou et al.
She is part of the Don’t Forget the Bubbles team and faculty at Queen Mary […] The post SGEM #404: Sitting on the Dock of the Bay-esian Interpretation of Therapeutic Hypothermia for Pediatric Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Therapeutic hypothermia after out-of-hospital cardiac arrest in children.
Background Therapeutic hypothermia, later rebranded as targeted temperature management, became a standard post-cardiac arrest therapy for comatose patients after two 2002 NEJM trials ( n=273 and n=77 ) suggested reducing core temperature to 32°C to 34°C markedly improved neurologic outcomes and survival.
Hypothermia for Neuroprotection in Convulsive Status Epilepticus. Case: Johnny is a […] The post SGEM#199: Therapeutic Hypothermia – What is it Good For? Hypothermia for Neuroprotection in Convulsive Status Epilepticus. Background: We have covered hypothermia a number of times on the SGEM. Reference: Legriel et al.
Induced hypothermia after cardiac arrest is also called “active temperature control” or “targeted temperature management.” TTM2 found no improvement in survival or neurologic outcome among patients randomized to cooling to a target of 33 °C, as compared to controls receiving fever prevention (e.g.
Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. Background: Hypothermia has been a mainstay of post-arrest care after the publication of two trials in 2002 that both suggested a benefit. This gives a NNT of 4.
It is useful to know that there are two kinds of weight curves: Descriptive , in which nearly all mothers and their children are included with few exclusion criteria, and Prescriptive , in which groups of women with pathologies that affect neonatal morbidity and mortality outcomes have been excluded. Eur J Pediatr 2016;175:1047-57.
Background Therapeutic hypothermia, later rebranded as targeted temperature management, became a standard post-cardiac arrest therapy for comatose patients after two 2002 NEJM trials ( n=273 and n=77 ) suggested reducing core temperature to 32°C to 34°C markedly improved neurologic outcomes and survival.
Exposure Expose the patient in a systematic manner while keeping remaining body areas covered e.g. 1 limb at a time, to reduce the risk of hypothermia. Proper stabilization and detailed communication with the burns centre are essential for optimal patient outcomes. Assess pupillary reaction to light.
Early work on TTM in 2002 showed benefit to cooling to 33 degrees Celsius, which subsequently influenced international resuscitation guidelines to recommend mild hypothermia at 32 degrees to 34 degrees Celsius in 2005. degrees Celsius. 5,6 In 2021, the TTM2 trial was published. degrees Celsius for 72 hours.
Induction of Therapeutic Hypothermia During Out-of-Hospital Cardiac Arrest Using a Rapid Infusion of Cold Saline The RINSE Trial (Rapid Infusion of Cold Normal Saline). Induction of Therapeutic Hypothermia During Out-of-Hospital Cardiac Arrest Using a Rapid Infusion of Cold Saline The RINSE Trial (Rapid Infusion of Cold Normal Saline).
Vaishnav Hyperthermia: abnormally high body temperature due to thermoregulatory failure Severe hyperthermia: temp greater than 40.5C stent, percutaneous nephrostomy) by urology or IR Hypokalemia evaluate for EKG changes assess for underlying cause and factors that may influence ability to replete (i.e.
This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), epinephrine ( SGEM#238 ) and IO vs IV (SGEM#231 and SGEM#340). .
The Annals of Emergency Medicine Podcast continues apace, with free monthly updates from the original research published in the journal: iTunes Link SoundCloud Link Likewise, the Annals of Emergency Medicine Journal Club has published several monthly installments: Predicting Outcomes in Pediatric Pneumonia: Are We Omnipotent or Incompetent?
Improving outcomes for patients with cardiac arrests has been an ongoing challenge in pre-hospital and in hospital medicine. SGEM#50 looked at a RCT published in JAMA 2013 looking to see if a vasopressin, steroids, and epinephrine (VSE) protocol for IHCAs could improve survival with favorable neurologic outcome compared to epinephrine alone.
However, no randomized trial has compared intravenous access to intraosseous access with a primary outcome of good neurologic function. Clinical Question: Is intraosseous vascular access in the pre-hospital setting for OHCA associated with better neurologic outcomes compared to intravenous vascular access?
Magnesium does not improve ROSC, survival, or neurologic outcomes, no matter the presenting rhythm (Level 3: no benefit). Patients with spontaneous hypothermia after ROSC unresponsive to verbal commands should not routinely be actively or passively rewarmed faster than 0.5° COR 2b, LOE C-LD. C per hour. COR 2b, LOE C-EO.
This has included the classic paper from Legend of EM Dr. Ian Stiell on BLS vs. ACLS ( SGEM#64 ), the use of mechanical CPR ( SGEM#136 ), and pre-hospital hypothermia ( SGEM#183 ). The key result was that significantly fewer patients had a favorable neurologic outcome in the IO group compared to the IV group.
Delays in providing adequate analgesia leads to poorer patient outcomes, prolonged ED length of stay and reduced patient satisfaction (17, 18). Multiple factors have been thought to contribute to oligoanalgesia (overcrowding, language barriers, age, gender, ethnicity, insurance status) (13-16).
This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), and epinephrine ( SGEM#238 ). The crew is asking if they should transport the patient with resuscitation ongoing?
Early Antibiotic Use and Neonatal Outcomes Among Preterm Infants Without Infections. To feed or not to feed during therapeutic hypothermia in asphyxiated neonates: a systematic review and meta-analysis. Eur J Pediatr. 2023 Apr 13. Patterns of parental online health information-seeking behaviour. Yudianto B, et al. 2023 Apr 13.
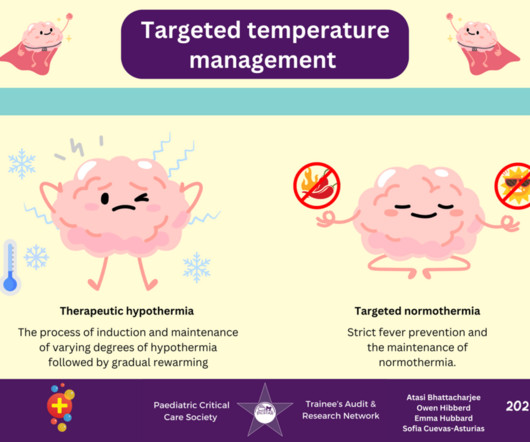
One-liner… Traumatic brain injury (TBI) is a leading cause of mortality and morbidity in paediatric populations, and fever is associated with worse outcomes. Therapeutic hypothermia involves the stepwise process of inducing a lower core temperature, maintaining this lower temperature, and then gradually rewarming over time.
The JET is treated by deepening sedation (to minimise exogenous and endogenous catecholamines), optimizing electrolytes and active mild hypothermia. These cases illustrate some of the common issues associated with each shunt type, but what does the evidence say about outcomes? What is the best option for repair?
The scheduled, usually elective nature of cardiac surgery lends itself to large scale outcome prediction and indeed, cardiac surgery has found its outcomes examined very closely over the past few decades. Likely driven by rewarming induced vasodilation and hypothermia induced diuresis they can be hypovolaemic.
Other states which could also affect sickling would be dehydration, acidosis, hypoxia and hyperthermia. High-quality studies in the SCT population are needed to clarify the health-outcomes as many studies are necessarily smaller or not able to be performed as rigorously. Clinical Outcomes Associated With Sickle Cell Trait.
Decompressive craniectomy * a bifrontal cranitoyomy is not recommended to improve neuro outcomes, which is a way of acknowledging the important DECRA trial. *
The post EM Quick Hits 35 – 10 Best Papers of 2021, Peripartum Cardiomyopathy, Crashing Asthmatic, Febrile Neutropenia, Anaphylaxis update appeared first on Emergency Medicine Cases.
trying harder and longer knowing they are enrolled in this study) Use of two different models of defibrillators may negatively impact the internal validity of this pilot study Certain baseline characteristics were not balanced, such as: prehospital intubation and Epinephrine administration.
Still, after a quick Google search, you realise that hypothermia potently affects potassium shift from the extracellular to the intracellular and extravascular spaces. Still, after a quick Google search, you realise that hypothermia potently affects potassium shift from the extracellular to the intracellular and extravascular spaces.
Broad-spectrum antibiotics (A) for septic shock are not inappropriate given the hyperthermia, tachycardia, and hypotension. Hyperthermia. As you attempt to examine the patient, he has a generalized, tonic-clonic seizure. What is your diagnosis, and what are your next steps in evaluation and management? 1 Fever is usually < 40C.
Alcohol withdrawal syndrome: improving outcomes through early identification and aggressive treatment strategies. fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
Older age, recurrent episodes of SBP, hepatorenal syndrome, hepatic encephalopathy, acute kidney injury (AKI), concurrent GI bleeding, and higher MELD scores are predictors of worse outcomes. Mild hypothermia is normal in patients with advanced cirrhosis; consider lowering threshold for fever to 37.8 coli (50-90% of cases).
This week we cover the POLAR RCT on hypothermia for neuroprotection in those with severe TBI. Take Aways: The data do not suggest that targeted hypothermia improves neurological function, reduces death, or reduces hospital length of stay as compared to normothermia. Welcome back to the “52 in 52” series. Bradycardia: 18.8%
The following Understanding and Managing Malignant Hyperthermia Training is designed to educate healthcare providers (HCP) on the genetic basis of malignant hyperthermia (MH). Nitrous oxide and xenon, while inhaled anesthetics, are not halogenated and have not been linked to malignant hyperthermia.
Patients can have excellent outcomes despite prolonged resuscitation. Some authors recommend not starting chest compressions in hypothermia unless there is no organized cardiac activity (e.g., 2 In reality you may start compressions before you confirm that hypothermia was the primary cause of cardiac arrest.
ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. Severe hypothermia not uncommonly has accompanying T waves inversions. Another frequent feature of hypothermia is atrial fibrillation (not seen in this case) Core temperature of this patient was 29,5 Celsius. There is SR.
Here we examine the most common category of cardiac arrests, which also have the worst outcomes: nonshockable rhythms. This variation contributes to a wide spectrum in outcomes. This series of posts reviews the data that can support clinicians in making the ultimate life-and-death decision: stopping CPR in the hospital.
These guidelines present the best available evidence to support clinical decision making in the prehospital setting when TBI care may have the most significant impact on outcomes; they also establish a research agenda for future investigations. This document is an update of guidelines first published in 2000, and then updated in 2007.
Mortality is high, between 16-43.5% , and neurological outcomes are generally poor amongst survivors. These poor outcomes are related to both the SRSE itself and as a result of the prolonged PICU stay. One study suggests remission in 6 out of 7 patients where it was used, but long-term clinical outcomes remained poor.
There is significant evidence in adults and developing in the paediatric population that TXA results in better outcomes if given early in patients with mild to moderate traumatic brain injury (TBI) and does not cause harm. Immediate Treatment One immediate medication to consider is tranexamic acid (TXA). General Medical Council.
Did the new treatment reduce the bad outcome so much so that the difference meets a statistical threshold? Two examples explain the challenge of using statistics to judge science In large studies, a tiny difference in outcomes—one that is not “clinically” significant can easily reach statististical significance.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content