This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
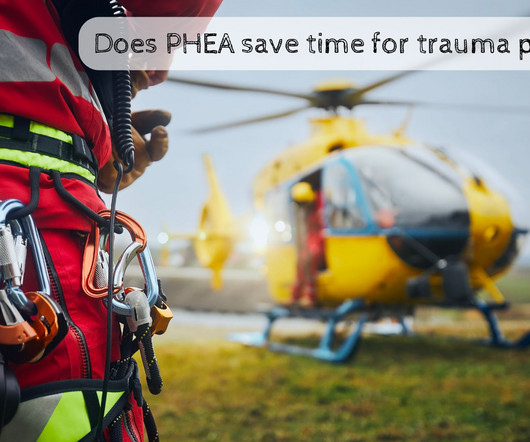
St.Emlyn's - Emergency Medicine #FOAMed How does pre-hospital emergency anaesthesia (PHEA) delivered by Helicopter Emergency Medical Services (HEMS) impacts trauma care timelines compared to emergency department RSI (EDRSI).
This is a series of articles on the duration of CPR for in-hospital cardiac arrest. hospitals each year, physicians receive no formal guidance or training on how long it should be performed. This series of posts reviews the data that can support clinicians in making the ultimate life-and-death decision: stopping CPR in the hospital.
Im currently in my third year of working in a rural district general hospital Accident and Emergency Department, and one of the things that has struck me most is the use of pre-hospital medicine. Ive always had a keen interest in pre-hospital medicine. Enter Nith Inshore Rescue!
This is part of a series of articles on the duration of CPR for in-hospital cardiac arrest. hospitals each year, physicians receive no formal guidance or training on how, when, or why it should be made. But first, a quick recap of what we know about all in-hospital cardiac arrests and shockable cardiac arrests.
hospitals each year, physicians receive no formal guidance or training on how, when, or why it should be made. This series of posts explores the available data that can support clinicians in making the ultimate life-and-death decision: stopping CPR in the hospital.
Background Out-of-hospital cardiac arrest (OHCA) primarily affects older adults. Methods Patients ≥18 years between 2015 and 2021 with a recorded location of either a nursing or care home from the ‘Out-of-hospital Cardiac Arrest Outcomes’ registry for England were included.
The work was done at a large teaching hospital and Level I trauma center in Australia. If you read the article closely, the trauma service at this hospital was staffed with a higher number of trainees after hours and on weekends than during office hours. What about the time of day? What gives?
It was so great to meet, hang out and talk ECPR with Paris’ SAMU ECPR leader Lionel Lamhaut last month in Montreal, a city we are actively trying to bring pre-hospital ECPR to, thanks to the relentless work of Lawrence Leroux. Come learn from some of the world leaders including Lionel himself, of course! Registration is 1,699 USD +tx.
If sepsis screening was shown to be beneficial in one hospital, would it be beneficial in another, with an entirely different set of caregivers? Article Background With all that as background, I was excited when I saw the article Electronic Sepsis Screening Among Patients Admitted to Hospital Wards in JAMA. 0.93; P < 001.
Naloxone and Patient Outcomes in Out-of-Hospital Cardiac Arrests in California. Background: We’ve discussed out-of-hospital cardiac arrest (OHCA) at least once or twice on the SGEM (see long list at end of blog). Clinical Question: Is naloxone administration in undifferentiated OHCA associated with survival to hospital discharge?
This month’s update is by the Emergency Department of the University Hospital of Heraklion, Crete, Greece. A randomised trial of drug route in out-of-hospital cardiac arrest. We used a multimodal search strategy, drawing on free open-access medical education resources and literature searches. Couper et al.
In a public letter, he highlighted the pressures of residency and stigma surrounding mental health, warning that there are other residents fighting a true life-and-death battleone that is waged both inside and out at the clinic/hospital. Elmhurst doctors’ strike ends as hospital, union reach deal. Thompson SL, Salmon JW.
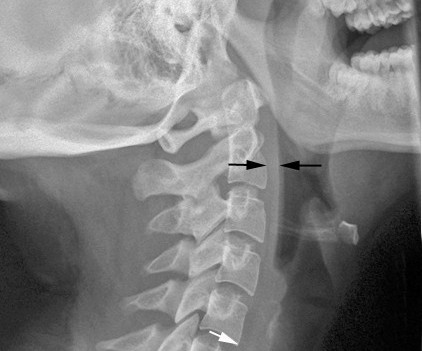
That being said, despite working in two very busy community hospitals with a high percentage of pediatrics visits, c-spine injuries are just not an issue I struggle with. As with everything that comes out of the PECARN group, this is a huge study, and is therefore one that everyone needs to know about.
In 2023, the Maryland Department of Health (DOH) adopted a standard for return to universal masking in healthcare facilities when hospitalizations with respiratory viruses (covid, influenza, or RSV) reach a level of 10 cases per 100,000 population. Maryland has a population of 6.3
For out-of-hospital cardiac arrest in particular, intravenous access can be difficult to establish, delaying the administration of epinephrine and other drugs and possibly worsening outcomes. During cardiac arrest, every second matters (at least potentially). Read more
Facts : A 28-year-old female is seen in the ED of Hospital A for recurrent bouts of severe, intermittent abdominal pain. 5 days later she is seen at Hospital B for similar symptoms. Another 10 days later she is seen at Hospital C , treated a third time for low sodium and discharged, this time with hydromorphone.
Developed by emergency medicine physicians at The Ottawa Hospital, this resource is tailored for learners and practitioners at all levels including medical students, residents, and staff physicians who […] The post Ottawa DVT PoCUS Handbook appeared first on EMOttawa Blog.
Case: The Chief of Emergency Medicine (EM) at a large urban hospital recently approached the AI Committee at Unity Health, intrigued by the CMAJ article describing the apparent success of CHARTWatch in detecting early signs of patient deterioration.
This is a decision that you and your hospital administration will have to work out. The average cost of a course of treatment in 2023 was $26,787 (ref 6). Can we justify such an expense if it doesn’t seem to save lives? At least until much, much better data comes along.
Approximately half of the failures occurred at the index hospitalization, whereas the remainder occurred over the one year of follow-up. These children spent less time in the hospital, were back to normal activity sooner, and required less analgesia. Adverse events were low and similar across each group.
St.Emlyn's - Emergency Medicine #FOAMed Recorded at the London Trauma Conference 2024, Richard Lyon shares insights from his powerful presentation on the importance of detailed case learning and debriefing both in hospital and pre-hospital settings.
This series provides evidence-based updates to previous posts so you can stay current with what you need to know. fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
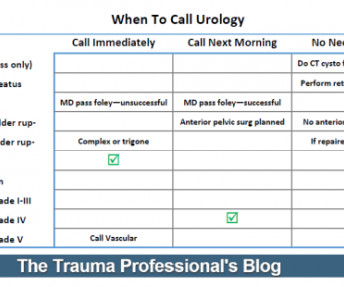
I’ve included a printable pdf file, as well as the original Microsoft Publisher file in case you want to make a few modifications to suit your own hospital. Here’s a reference sheet formatted at a 3×5 index card that you can keep in your pocket. When to call Urology reference card (pdf)
As only a minority of hospitals even provide ordinary physical therapy to mechanically ventilated patients on a routine basis, the advisement is largely symbolic or aspirational. Hospital Mortality (n~2,930): RR 1.01, CI 0.84 In a March 2025 guideline update, the major U.S. ICU Mortality (n~4,730): RR 0.98, 95% CI 0.85
Eckler, MD discuss the January 2025 Emergency Medicine Practice article, Alkali Exposure: An Evidence-Based Approach to Diagnosis and Treatment Patient Demographics and Case Scenarios: Types of patients prone to alkali exposure Causes and scenarios leading to alkali exposure (e.g.,
Assessment A code of practice for confirmation of death exists, however, each hospital may have its own protocols which you must familiarise yourself with. The patient must be observed for a minimum of 5 minutes to establish irreversible cardiopulmonary arrest has happened.
Instead, he left the hospital — only to be found dead at home 36 hours later. For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chest pain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1.
Getting there includes an obvious problem: what happens when the physician leaves the hospital? Other surgeons may be available in the hospital during the daytime, although they may have other responsibilities keeping them busy. For emergency physicians, there are generally several on duty, so one will not be missed too much.
St.Emlyn's - Emergency Medicine #FOAMed How does pre-hospital emergency anaesthesia (PHEA) delivered by Helicopter Emergency Medical Services (HEMS) impacts trauma care timelines compared to emergency department RSI (EDRSI).
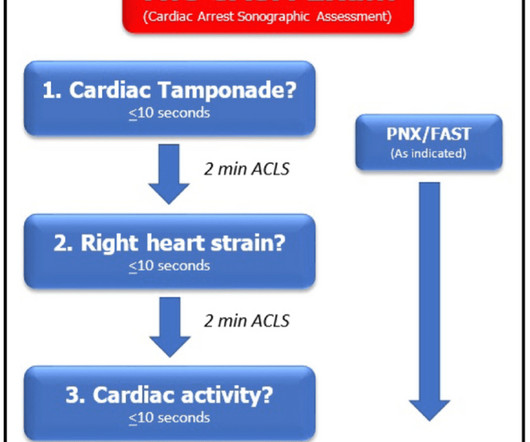
Rapidly intervened-upon cardiac tamponade in PEA during cardiac arrest has significantly higher hospital discharge rates. survival to hospital discharge rate. Evidence of right heart strain is important but the evidence of fibrinolysis during arrest is mixed with many studies showing no 30-day mortality benefit to lysing during a code.
Elizabeth Wharff was the director of emergency psychiatry at Boston’s Children’s Hospital in the late 1990s when she became concerned about what was, then, a new problem. They would be the least difficult and disruptive, the least strain on the hospital staff,” Dr. Wharff explained.
Changing the way surgeons prepare for surgery can reduce water consumption in hospitals A recent study by the Campus Bio-Medico in Rome has revealed an astonishing truth: changing the way surgeons prepare for surgery can drastically reduce water consumption in hospitals.
They carry out functional assessments (in a hospital or in a home environment), identifying areas where the patient may require extra aid. The Community Care (Delayed Discharge) Act 2003 details how NHS hospitals should communicate with social care about discharges of inpatients. This allows patients to receive fully funded care.
Dr Penny Wilson, GP Obstetrician ( @nomadicgp on X ), joined us recently at a GSA-HEMS Education Day to discuss key peri-partum emergencies in the context of pre-hospital and retrieval medicine. The recognition and management of cord prolapse, breech delivery and shoulder dystocia are discussed in her talk, now on our YouTube channel.
I would discourage the use of propofol because it is difficult to titrate outside the hospital and may contribute to hypotension. Finally, don’t assume that you will accompany the patient (and possibly their limb) back to the hospital. Paralytics, sedatives and analgesics are essential.
This problem was associated with a significantly longer ICU stay and a somewhat longer overall hospital stay. They studied a series of 79 of their patients who were treated with a halo. A full 66% had problems with their swallowing evaluation. Bottom line: Suspect dysphagia in all patients with cervical fractures, especially the elderly.
The "good news" — is that after an extended hospitalization, the patient was finally discharged home, and doing well. = . = The H ISTORY in T oday's C ASE: The patient in today's case is a teenager who presented to the ED ( E mergency D epartment ) in cardiac arrest after electrocution.
Unfortunately, they were very conservative, recommending days of bedrest, extended NPO status, very frequent blood draws, and a lengthy hospital stay. Many hospitals, including mine, developed less conservative management routines, noting that children nearly always tolerate liver and spleen injury better than adults.
A recent Massachusetts General Hospital study involved a larger group (97 patients with 110 fixators). Consult your radiologists and physicists to develop a policy that is specific to the scanners used at your hospital. Most MRIs were performed to evaluate the cervical spine. There were no adverse events. Most were performed on a 1.5T
Getting them to the scene will always take extra time since they are typically hospital-based. Look at your local resources and the logistics imposed by the environment, traffic, hospital, and other factors. In contrast, the prehospital providers are already present and are used to working in an austere environment.
References: “ The VIP Syndrome”: A Clinical Study in Hospital Psychiatry. Order the same tests you usually would, use the same consultants, and take control of all of their recommendations, trying to do things your usual way. This will provide the VIP with the best care possible, which is actually the same as what everybody else gets.
This allowed US hospitals to stock the drug to ensure quick treatment of suspected severe cases, rather than having to ship it from the CDC under the prior expanded-access protocol (Thomas 2023). Higher Rates of Misdiagnosis in Pediatric Patients versus Adults Hospitalized with Imported Malaria. June 28, 2023. J Travel Med.
compared the effects of these two among the acute gastroenteritis children and reported that the use of ORT was associated with shorter hospital stay and increased patient satisfaction. demonstrated that use of ORT was characterized by shorter stays at the hospital. AtherlyJohn et al. A systematic review by Freedman et al.
Paracentesis performed within 12 hours was associated with lower in-hospital mortality and shorter length of stay when compared to paracentesis performed within 12-72 hours (13% compared to 27%). Delayed paracentesis is associated with increased in-hospital mortality in patients with spontaneous bacterial peritonitis.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content