This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
risk of C Spine injury) Altered Mental Status (GCS 3-8 or U on AVPU) Abnormal ABCs on exam Focal Neurologic Deficits (paresthesia, numbness, weakness) Not Negligible Risk (2.8% Moral of the Morsel Anatomy Matters: Pediatric patients have unique C-spine anatomy, which predisposes them to different injury patterns than adults.
Background: We have covered headinjuries including concussions multiple times on the SGEM. This has included looking at the Canadian CT Head Rules/Tools ( SGEM#106 , SGEM#266 , and SGEM#272 ). This has evolved due to recognition of some of the adverse effects of immobilization as well as limitations to its benefits.
She is the cofounder of FOAMcast and a pulmonary embolism and implementation science researcher. Dr. Westafer serves as the Social Media Editor and a research methodology editor for Annals of Emergency […] The post SGEM#331: Should Patients with a Concussion be told to Walk this Way! Reference: Varner et al.
Case: It’s a busy night in the emergency department, your next patient is a well appearing 70-year-old man, presenting after a mechanical fall from standing with loss of consciousness. The Canadian CT Head Rule [2] is a clinical decision instrument to help you decide if a patient with a mild headinjury requires a CT head.
Researchers utilized two bias tools in an attempt to assess bias: The Cochrane Risk of Bias Tool was used for RCTs. The “usual care intervention” was not well-defined. However, the definition of “social” activities was not well defined. Investigators performed a comprehensive search of multiple databases.
The bottom line was that this paper opens the door for further research to try to narrow the criteria in the CCHR to further reduce unnecessary head CT imaging in the emergency department. We also recently reviewed a paper that looked at increasing the CCHR age criteria from 65 years of age to 75 years of age ( SGEM#266 ).
Emergency physicians have become leaders in achieving cost efficiency in health care, predominantly through implementation of new processes and research findings, enabling us to achieve significant financial savings. Pediatric Emergency Care Applied Research Network headinjury clinical prediction rules are reliable in practice.
While well evaluated, you see the residents go back to the shop floor and struggle to apply any of the lessons that the group agreed had been take homes from the previous sim session. How do they do it so well?” This demands more research.” Well done”……. he thought. Deep breath. “OK OK guys that was great.
Dr. Varner’s research interests are in concussion and pregnancy care in the ED. Case: An 18-year-old female presents to the emergency department (ED) after falling off a moving snowmobile and hitting her head on the ground. An issue that often comes up with minor headinjuries is do we need to get advanced imaging.
We have mentioned the Glasgow Coma Scale in multiple delicious morsels: Minor closed headinjuries in <3 month olds and in the rebaked morsel , Blunt cerebrovascular injury , Cerebral edema in DKA , Pediatric Trauma Pitfalls , and Carbon monoxide poisoning. Predicting outcome in individual patients after severe headinjury.
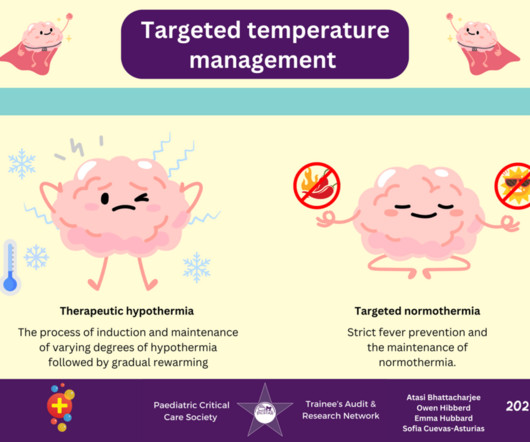
One-liner… Traumatic brain injury (TBI) is a leading cause of mortality and morbidity in paediatric populations, and fever is associated with worse outcomes. A 12-year-old boy presents with a significant headinjury following a road traffic accident. Should we aim to prevent fever, or should we cool patients?
At the time, there was a debate about whether the procedure should be done immediately versus waiting until the patient was well-resuscitated. The first is from an international research group that searched the usual databases and initially found 921 records. However, the same question arises: do it early or wait a while?
Patient data anonymized when presented to adjudication committee to avoid detection bias Well-balanced patient characteristics between groups. Included traumatic and nontraumatic brain injuries. 8 Author’s Conclusion: “In patients with acute brain injury, a single ceftriaxone dose decreased the risk of early VAP.” .;
It is a free, critical appraisal blog and podcast that try to cut down knowledge translation gaps of research to bedside clinical practice. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. Reference: Rowell et al.
CRASH-3 TRIAL COLLABORATORS This international, multi-center, randomized, placebo-controlled trial looked at the effects of TXA on headinjury-related death, disability, and adverse events in adult patients with TBI. The primary outcome was headinjury-related death in-hospital within 28 days of injury.
11,12 It is important to limit the development and cancer risks of radiation on children while effectively screening for serious and potentially life-threatening injuries. References Coalition for National Trauma Research (CNTR). Stiell IG, Wells GA, Vandemheen KL, et al. Trauma Statistics and Facts. Accessed 02/01/2025.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content