This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This demands more research.” Mental practice: a simple tool to enhance team-based trauma resuscitation. The ED team had just finished an in situ simulation where the focus was on rapid sequence intubation (RSI) in headinjury, and using the new intubation checklist. I’d better come back tomorrow.” 2016 Mar;18(2):136-42.
One-liner… Traumatic brain injury (TBI) is a leading cause of mortality and morbidity in paediatric populations, and fever is associated with worse outcomes. A 12-year-old boy presents with a significant headinjury following a road traffic accident. Should we aim to prevent fever, or should we cool patients?
At the time, there was a debate about whether the procedure should be done immediately versus waiting until the patient was well-resuscitated. The first is from an international research group that searched the usual databases and initially found 921 records. However, the same question arises: do it early or wait a while?
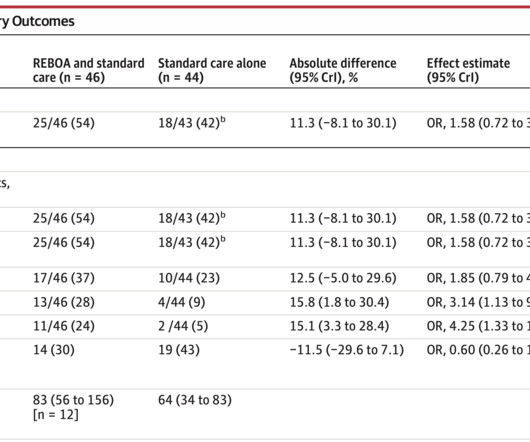
Early expeditious definitive hemorrhage control is a major focus in trauma resuscitation. Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial [published online ahead of print, 2023 Oct 12].
The primary outcome was 30-day mortality with secondary outcomes looking at 24 hour in-hospital mortality, blood resuscitation at 6 and 24 hours, incidence of multiorgan failure, ARDS, nosocomial infection, early seizures, PE/DVT, crystalloid resuscitation after 24 hours, and the incidence of coagulopathy.
It occurs when a mechanical force to the head injures the brain. This can be from the brain hitting the skull, shear forces from sudden acceleration and deceleration, or direct injury at the point of impact. The severity of headinjuries can be classified according to the GCS.
10 Standardizing evidence-based care ensures that every child, regardless of where they present, receives optimal initial resuscitative care. Emergency physicians need to make fast-paced decisions regarding imaging to evaluate for serious injuries. References Coalition for National Trauma Research (CNTR). Accessed 02/01/2025.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content