This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
CRYSTALLOIDS Too much crystalloid resuscitation in traumatic hemorrhagic shock can increase dilutional coagulopathy, as well as increase morbidity and mortality Bickell WH et al. I recently gave a talk on the initial management of trauma patients with hemorrhagic shock. vs SBP target <90mmHg which resulted in a mortality of 33.4%
They cautioned against the use of TXA in the setting of whole-blood resuscitation. Specific ones that come to mind are shock, long bone or spine fractures, and TBI. Reference: Does whole blood resuscitation increase risk for venous thromboembolism in trauma patients? increase in risk. Bottom line: A lot is going on here.
His CT scan showed extensive cranial fractures, traumatic subarachnoid haemorrhage, and intraparenchymal haemorrhage. A 12-year-old boy presents with a significant head injury following a road traffic accident. At the scene, his lowest GCS was 5 (E1V2M2). He went to theatres for an ICP (intra-cerebral pressure) bolt.
St.Emlyn's - Emergency Medicine #FOAMed Day 2 of the London Trauma Conference delivered impactful discussions on trauma care innovations, including advanced resuscitation strategies, rib fracture management, and prehospital interventions.
Please consider a donation to ensure EM Cases continues to provide you high quality Free Open Access Medical Education here: [link] The post EM Quick Hits 60 Post-Tonsillectomy Hemorrhage, Post-CABG Infections, Bougie Tips, Pelvic Fracture Bleeds, Debriefing: Why, When & How appeared first on Emergency Medicine Cases.
Most commonly caused by fracture or dislocation of vertebrae. While we may allow permissive hypotension in damage control resuscitation of hemorrhagic shock, in neurogenic shock you should maintain an age-appropriate blood pressure. This leads to descending sympathetic tracts being disrupted.
Whether you’re interested in orthopaedics or not, knowledge of basic fracture management can be useful in any ED. Examination of a fractured limb Most patients will be in a lot of pain. If the limb is pale and pulseless this needs urgent referral to vascular as well as orthopaedics and the fracture needs reducing immediately.
Critically ill patients requiring resuscitation often present with many challenges including the ability to secure safe, sterile, fast, and reliable intravenous (IV) access. This can often lead to significant delays in proper resuscitation. Studies reviewed landmark-based CVC compared to IO; using IJ, subclavian, and femoral CVC sites.
just be careful with pelvic fractures or any femoral arterial punctures/ devices. lactate-targeted fluid resuscitation on regional, microcirculatory and hypoxia-related perfusion parameters in septic shock: a randomized controlled trial. 14,15 You might use a passive leg raise, which carries a roughly 250cc fluid challenge.
In this EM Quick Hits podcast: Justin Morgenstern on fluids in pancreatitis, Leeor Sommer on nasal fractures, Christina Shenvi on delirium, Sheldon Cheskes and Rohit Mohindra on Dose VF, and Noor Khatib and Kari Sampsel on intimate partner violence.
Most common traumatic injuries are fractures, TBIs, and thoracic or abdominal injuries. Fluid resuscitation target and fluid Fluid resuscitation is one of the most important parts of management; goal is to increase intravascular volume and ensure end organ perfusion. Always consider trauma and toxic exposure in the burn patient.
Look for the light bulb sign and always evaluate with scapular 'Y' view Lateral ankle fractures are classified by the Weber Classification, which is based on fracture location relative to the tibiotalar joint line A Jones fracture is a fracture at the 4th/5th metatarsal articulation. C above historical average.
The post EM Quick Hits 30 Scaphoid Fracture, Therapeutic Hypothermia, HEADS-ED, Pelvic Trauma, Kratom, Femoral Lines appeared first on Emergency Medicine Cases.
Be careful with fluid resuscitation in renal transplant patients who can be at risk for volume overload. Validity Evidence for a Team-Leading Assessment Tool in Pediatric Emergency Resuscitation Using Video Review (Hartwell et al.) Assessed and provided feedback of pediatric resuscitations based on video review.
The resuscitation equipment is not on par with the OR, and one never knows exactly how long the procedure will last. Reference: Preperitoneal packing versus angioembolization for the initial management of hemodynamically unstable pelvic fracture: A systematic review and meta-analysis. Pay attention to hemodynamic stability.
Ben has a possible skull fracture and has been intubated, but his oxygen requirement is minimal. Tragically, several attempts at resuscitation upon arrival at the emergency department were unsuccessful. You are the Paediatric doctor on call and receive a call for an incoming patient to the emergency department. His name is Ben.
The trauma will be an open book pelvic fracture with hypotension and a positive FAST. The resident will need to immediately evaluate the patient with hyperkalemia and give appropriate medications or they will decline. As they are pushing the medications, a Trauma Level One will be called.
Absolute contraindications of prone positioning are severely increased intracranial pressure as positioning of the head in prone position can partially obstruct cerebral venous drainage, as well as unstable spinal fractures because the manipulation while repositioning a patient may lead to further injury (Guerin et. 2020; Koulouras et.
Depending on the height of the child and the height of the car, the initial impact will cause a femur fracture, a pelvic fracture, or direct abdominal trauma. Resuscitative Thoracotomy in Children In a 40-year review of ED thoracotomy, Moore et al. Resuscitative thoracotomy for blunt trauma has a dismal prognosis in children.
1 Though hydrocortisone is often included in ‘crash carts,’ the most recent consensus on cardiopulmonary resuscitation (CPR) has a weak recommendation against the use of corticosteroids during CPR. Consider the other complications of systemic steroids: weight gain, cataracts, fractures, and neuropsychiatric events.
He sustained a femur fracture, splenic laceration, and blunt head trauma – the so-called Waddell’s triad. Resuscitative Pearls Our goal here is damage control. Otherwise, resuscitate, identify the bleeding source, and slow or stop the bleeding with blood products or surgery. Rib fractures on CXR predict pulmonary contusions.
Resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. Intra-Aortic Balloon Occlusion to Salvage Patients with Life-Threatening Hemorrhagic Shocks from Pelvic Fractures J Trauma 2010; 68(4): 942–8 (full article free text) 3. Stannard A, Eliason JL, Rasmussen TE. Martinelli et al.
Radiographs from children with fractures, or disease processes affecting bone growth, were excluded. 2004) Positive end expiratory pressure during resuscitation of premature lambs rapidly improves blood gases without adversely affecting arterial pressure. Probyn, M.E., Hooper, S.B., Dargaville, P.A., McCallion, N., Crossley, K.,
Sameer Sharif (Hamilton Health Sciences, Hamilton, Ontario) and Dr. Sophie Ramsden (Emergency Medicine Resident, McMaster University, Hamilton, Ontario) Why it Matters Major trauma patients sometimes decompensate after initial resuscitation. ICU has admitted the patient while she awaits OR later today to stabilize the spine.
US GUIDED ULNAR NERVE BLOCK [BLOG]: Boxer's fracture need a reduction? Consider an ultrasound guided ulnar nerve block. Check out the case here and be sure to watch the video tutorial from 5minsono.
CT HEAD Bilateral hemorrhagic contusions, left subdural hematoma with mass effect, scattered subarachnoid hemorrhage, occipital bone fracture and venous thrombosis adjacent to fracture site. This does not deviate from general resuscitation principles for acute hemorrhage.
In this episode we talk to Joseph Mathew, one of the authors of a great new article on a novel technique for tamponade of bleeding related to pelvic fractures. Delaying urinary catheter insertion in the reception and resuscitation of blunt multitrauma and using a full bladder to tamponade pelvic bleeding.
Blunt trauma can cause rib fracture or dislocation that may injure the visceral pleura. PPV, rib fractures, and decreased GCS were predictive of conservative management failure [23]. Unsuspected tension pneumothorax as a hidden cause of unsuccessful resuscitation. Resuscitation. Rojas R, Wasserberger J, Balasubramaniam S.
CPR (cardio-pulmonary resuscitation) is a technique used to keep victims of sudden cardiac arrest and other emergencies, alive and to prevent brain damage until more advanced medical professionals arrive. The following CPR Refresher Course educates healthcare providers (HCP) on the basic principles of CPR.
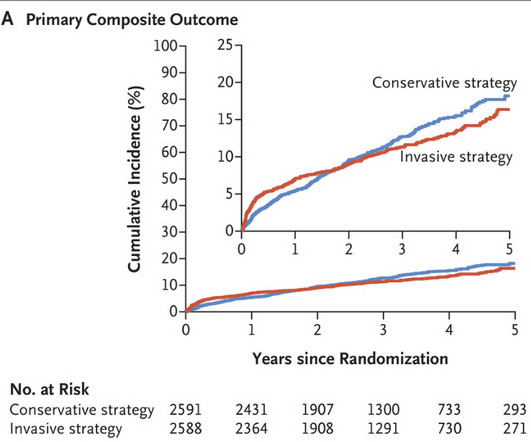
The primary endpoint was a composite of 5 bad things: death due to cardiovascular causes, MI, unstable angina, heart failure, or resuscitated cardiac arrest. When these partial blockages are just there (stable), we don’t know that they will fracture and cause MI. Here was the result. After a median follow-up of 3.2
Splint to reduce fracture bleeding. We are not always as fastidious as we should be because of the universal availability of blood products. Use direct pressure or direct suture ligation for external bleeding. Aggressively use damage control surgery. Don’t go for a definitive laparotomy which may take hours.
Ensure that you have a solid understanding of the core subjects, including emergency medicine, clinical skills, critical care, resuscitation, and trauma management. Review the Exam Syllabus: Carefully go through the exam syllabus to identify the key topics and areas that will be tested.
Establishing reliable vascular access is absolutely critical for ED patients requiring resuscitation, airway management, or medication administration. IOs can be used both for resuscitation, medication administration, and for laboratory testing, but there are a few important considerations.
Broadstock and Ramachandran Nerve blocks should be a part of your multimodal analgesia toolbox in the ED Basic Equipment: antiseptic cleaner barrier protection needle (EchoBlock needs are specifically designed for regional anesthesia and available in our ED) anesthetic typically 0.5%
The most common injuries seen in these younger patients are growth plate fractures and ligamentous injuries. You more often will see vertebral body and arch fractures as opposed to the growth plate fractures and ligamentous injuries in the younger children. Resuscitate with volume and blood. than it is spinal shock.
Through this role, as an observer, I was able to experience various pre-hospital emergencies; the most common scenarios I attended were cardiac arrests, but I also attended trauma patients at the scene of road traffic accidents, fractures in a wilderness medicine setting, anaphylaxis, and many others.
Clinically, your enthusiasm for providing maximal quality care needs balanced against rescue practicalities and a hostile environment (very different to your warm, dry resuscitation bay) – the cold makes all veins disappear…and you may be the only clinician responder at the scene.
However, believers in this superstition will perceive crazier shifts if the word is uttered so you probably shouldn’t say it, or use cautiously Full moons have no impact on ED, EMS, or HEMS volumes or acuity.
In fact, one of my surgeon grandfather's ortho buddies (perhaps with the help of some lunchtime martinis) took a look at the x-rays of my Boxer's Fracture and snapped it back into place without any analgesia or procedural sedation, casted me, and sent me home. 1950s & 1960s Resuscitation Research. Still no pain medicine.
The two most common complications of VP shunts are malfunction (due to obstruction, fracture, or kinking) or infection. The Huber needle is not a resuscitative line. Vascular Devices: assume the line is not functional, and use another to resuscitate, especially in port-a-caths. He is in compensated shock.
Treatment for burns should focus on fluid resuscitation as appropriate based on your institution’s burn protocol per Brooke, Parkland, Rule of 10s etc. Lastly, vessels can be damaged by internal burns, which may lead to poor perfusion and delayed complications as thrombosis or third spacing. His ECG was unremarkable.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content