This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Earlier this year, I wrote a series of posts on the two commonly used pelvic fracture interventions: preperitoneal packing (PPP) and angioembolization (AE). To sum up, both are equally effective in controlling hemorrhage, but the hospital costs for patients undergoing angioembolization are significantly less. DVT, and 1.9%
Many vertebral fractures can be treated non-operatively. So I would like to concentrate on some papers that examined the use of back braces on patients who underwent pedicle screw fixation of their thoracic and/or lumbar spine fractures. I found two systematic reviews and a ten-year prospective clinical trial.
This places a significant responsibility on the EM physician to diagnose and treat fractures. Specifically, EM physicians should be able to recognize fractures that will likely require operative management and facilitate close follow up, such as a Maisonneuve fracture. 2) It is a specific type of a Weber C ankle fracture.
In this series, I will review the two major techniques for addressing troublesome bleeding from pelvic fractures. In the last post in the series, I’ll discuss a paper in press that compares the efficacy and hospital charges of the two techniques. As I continue to preach, going anywhere but the OR is dangerous for the patient.
Ultrasound‐Guided Serratus Anterior Plane Block (SAPB) Improves Pain Control in Patients With Rib Fractures. This topic is important because of the high incidence of rib fractures in trauma patients and their association with increased morbidity and mortality. Ultrasound Med. 41, 2695–2701 (2022). Why do we care? SD 3.28) and 6.5,
Introduction Clinical Definition An open fracture is when the broken bone breaks through the skin or any other body cavity that is open to the outside, including those through the rectum or vagina. This is especially vital when addressing the issue of a fracture, adequate soft tissue coverage or blood vessel injury.
This necessitates an inter-hospital transfer that is subject to scrutiny by the trauma performance improvement program of both trauma centers. The work-up from the referring hospital can be re-evaluated. In some hospitals, orthopedics may choose to place a traction pin to provide initial fracture management.
He initially presented to an outside hospital where he was told he had an “ankle” fracture and was splinted with a short leg posterior splint. Mildly displaced oblique fracture involving the proximal fibular metaphysis. Otherwise, most cases require operative repair. The patient was sent for radiographs. J Emerg Med.
and get 20% of all orders at [link] Emergency Department Management of Rib Fractures Author: Patrick Maher, MD Episode Outline: Why rib fractures? and get 20% of all orders at [link] Department Management of Rib FracturesAuthor: Patrick Maher, MDEpisode Outline:* Why rib fractures?*
Ben has a possible skull fracture and has been intubated, but his oxygen requirement is minimal. A retrospective cohort analysis of the ED portion of the National Hospital Ambulatory Medical Care Survey from 2006 to 2009 in the US revealed that less than one-half of patients undergoing ETI in the ED received sedative drugs while in the ED.
Background During closed reduction of displaced distal radius fractures, physical examination is used to determine the need for further manipulation before radiographic confirmation and cast application. The secondary outcomes were time to complete reduction and treatment plan at ED discharge (conservative or operative repair).
Many clinicians don’t consider IO placement while others consider it a last resort or only a pre-hospital procedure. Intravenous vs.intraosseous vascular access during out-of-hospital cardiac arrest – protocol for a randomized clinical trial. PMID: 33350794 10 Meilandt C. Resusc Plus. 2023 PMID: 37502742 11 Schwalbach KT et al.
For mid-shaft femur fractures, traction appears to may reduce blood loss and pulmonary complications, but the available data is very scarce. Guidelines also support not administering HTS in the pre-hospital setting, yet the available data is weak. What do we do at UC?
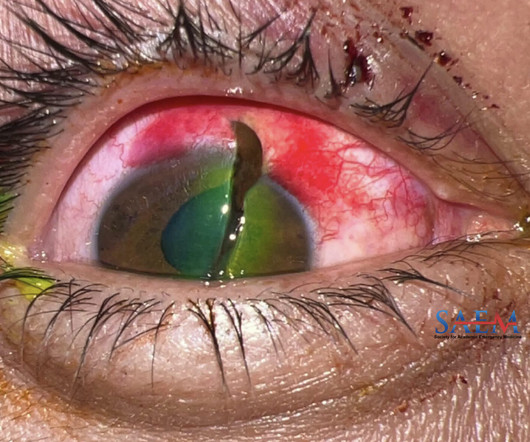
A 32-year-old male with no significant past medical history presented to the emergency department (ED) from an outside hospital for further management of right eye pain and vision loss sustained after he was struck by a metal wire while at work. Laboratory Data CT Orbits/Sella w/ IV Contrast : No acute orbital fracture.
A more inquisitive approach would seek to understand why the educational bargain feels more fractured now despite ACGME work hours being more “protective” than ever before. The analogy of a physical hospital expanding from its original isolated ward to become an interconnected quaternary care center may help.
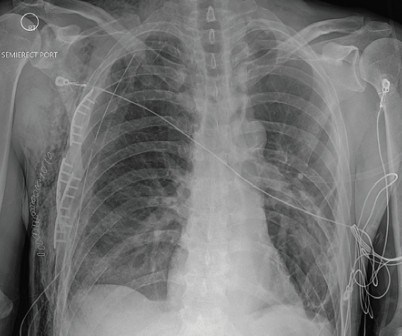
Case FIGURE 1: Chest X-ray of multiple rib fractures (arrows). The chest X-ray showed multiple displaced right rib fractures and chest wall subcutaneous emphysema without definitive evidence of a pneumothorax, as well as right lower lobe atelectasis versus contusion (Figure 1). Click to enlarge.) Click to enlarge.) Click to enlarge.)
The Bubble Wrap Plus is a monthly paediatric journal club reading list from Anke Raaijmakers, working with Professor Jaan Toelen and his team at the University Hospitals in Leuven. Post-operative pain in children: Comparison of pain scores between parents and children. Can’t get enough of Bubble Wrap? 2023 Apr 24. Eur J Pediatr.
The clavicle is one of the most commonly fractured bones in the human body. Every year, approximately 332,000 people in the United States suffer from a clavicular fracture. The clinician should note the fracture site (either via palpable landmark or ultrasound visualization). Click to enlarge.) for the ED clinician.
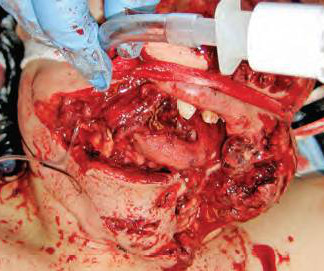
Laryngotracheal trauma has been cited as accounting for less than one in 100,000 hospital admissions. Fracturing the larynx requires considerable force, and the great majority of fractures are from blunt high-velocity trauma. Is there an open neck wound or palpable cartilage fracture?
A search for Brazilian Butt Lift (BBL) on any social media platform will yield thousands of before-and-after images, faja sales, operating room videos, recovery tips, and patients praising their plastic surgeon. 1 The Rise of the Miami BBL An entire industry has emerged around gluteal AFTs in Miami.
This time the team from Bristol Royal Children’s Hospital ED tell us what is new in the world of paediatric literature… Led by Dr John Coveney a Paediatric Emergency Medicine Trainee in Bristol who has revived The Journal Club at Bristol Royal Children’s Hospital ED on a monthly basis. 2023 Mar 30;110(4):432-438.
Casey currently splits his time between Broome, a small rural hospital in the remote Kimberley region of Western Australia, and a large tertiary ED in sunny Perth. Do they need surgery, an ERCP or just analgesia and non-operative care? He is also now a fully-fledged “sonologist”. He has been on the SGEM#369 , SGEM#326 and SGEM#217.
In our case, the patient had a CT of the head, cervical spine, and chest, abdomen, and pelvis with intravenous contrast demonstrated a C2, C7 compression fracture with significant bowel edema (Figure 4), and was taken to the operating room for left arm disarticulation, left below knee amputation and right above knee amputation.
All things Pre Hospital Ketamine – Minh Le Cong Key point: patients remember if you manage their pain well. Spinal fractures occur in 2% of all major trauma. Unstable spinal fractures occur in all major trauma 0.7%. We have also recorded a three interviews already which will feature in future podcasts.
Notable Diagnostics CBC : unremarkable, BMP : unremarkable X-ray imaging of the left hand, wrist, and forearm: chronic degenerative changes without acute fracture or bony abnormality. Hospital Course The patient was initiated on a therapeutic heparin drip in the emergency department with vascular surgery consultation.
Scottish Mountain Rescue (SMR) is an umbrella organisation, with teams the final decider of how they operate. Your skills as a doctor need to be different to your hospital role or abilities. Team equipment, procedures, training schedules/frequency, and skill mix vary between teams greatly. What illnesses or injuries do we see?
The most common injuries seen in these younger patients are growth plate fractures and ligamentous injuries. You more often will see vertebral body and arch fractures as opposed to the growth plate fractures and ligamentous injuries in the younger children. Axial load can cause burst fracture, so someone that dives into a pool.
Assess for head and neck trauma : A 2014 study out of NYU/Bellevue Hospital found that 39% of patients who frequented the emergency department with acute alcohol intoxication had a moderate to severe brain injury over a three-year period. Check that clavicles are intact and that there are no obvious rib fractures or spinal step-offs.
" [Coroners Society] King Richard I (the Lionheart) needed vast sums of money for the Third Crusade, operation of the kingdom, and for his ransom fro m Duke Leopold of Austria. All efforts to identify the decedent by hospital staff, law enforcement agencies or social service agencies should be well documented in the medical records.
Still, except for the public hospital, other hospitals did little emergency work and would have unattended first aid or treatment room in which one could meet one's physician or have an intern provide care in the meanwhile. Rebuilding of EDs in proximity to Radiology, Blood Bank, OR, and ICU, becoming organic to the hospital.
X - ray : Many times, next step will be to get an X-ray to look for associated fractures. Definitive treatment is joint wash out in the Operating Room. It provides additional information about any associated fractures. It is important to note that the absence of these findings does not rule out a traumatic arthrotomy.
Depending on the height of the child and the height of the car, the initial impact will cause a femur fracture, a pelvic fracture, or direct abdominal trauma. Withholding or termination of resuscitation in pediatric out-of-hospital traumatic cardiopulmonary arrest. Pediatrics. 2014 Apr;133(4):e1104-16.
James and Casey are used to this kind of stuff (although Casey’s mostly in-hospital and has even got a CT scanner…James is used to working out of a tent wearing just rabbit skins). Allocate someone to activate ambulance, other clinical personnel, notify local hospital and give retrieval services a head’s up. The CAT will hurt.
Physical examination should always include an attempt to ambulate the child unless there is an obvious contraindication noted immediately (eg open fracture). Management is orthopedic consultation for operative stabilization [12]. Strength and range of motion of both lower extremities should also be examined [2]. 2012;97(5):185-193.
After a several week NICU stay for prematurity, the infant has been generally healthy and this is his first trip back to the hospital since discharge. Obtain shunt imaging (“shunt series,” CTH non-con) Shunt series shows no migration of the shunt catheters or fractures of the tubing.
4 Pain is the most common reason for presentation in the early post operative period. 5 Highest risk of dislocation early in the post operative course due to laxity of the soft tissue after surgery. 6 Hip flexion or adduction in the early post-operative period can cause atraumatic dislocations (typically avoided for 6 weeks post-op).
In a small study involving 79 hospitalized children, PCT was found to be elevated in bacterial infections, with a decrease after appropriate antibiotic therapy, and decreased in viral infections [24]. This finding was not significantly different among operators with different levels of experience, or between adults and children.
We have teamed up with the team from the Emergency Department at Bristol Royal Hospital, who have used this as a springboard for their journal club. (It’s The hospital is the Paediatric Major Trauma Centre for the South-West. It’s a great idea and maybe something for other centres to copy!) in lower-resource settings.
Taylor and Shaukat of Emory and Coney Island Hospital respectively for their efforts in peer reviewing this huge topic. Nachi: And as a brief aside, before we continue… Missed appendicitis is one of the three most common causes of emergency medicine malpractice lawsuits - with MI and fractures being the other two.
A trans-esophageal echocardiogram showed a normal ejection fracture, normal right ventricular function, and no vegetations. Your patient ultimately is diagnosed with a spinal epidural abscess requiring operative care. Clinical impact: The patient’s DVT ultrasounds were negative. J Am Psychiatr Nurses Assoc. 2023;29(6):470-476.
Her Glasgow Coma Scale (GCS) is 14 (3E-5V-6M), and she arrives in a cervical collar placed pre-hospital. How should pelvic fractures be identified in unstable trauma patients? Pelvic fractures can involve disruptions in any of the bony or ligamentous structures of the pelvic ring. 2 Vertical shear fractures are also unstable.
Reports of a pre-hospital deformity, “popping” sensation, or reduction attempts should raise suspicion for a spontaneously reduced knee dislocation. CTAs have the added benefit of also further evaluating the surrounding osseus structures for associated fracture.
Neonatal observational scales have been validated in the intensive care and post-operative settings; ED-specific quantitative scales are lacking. CRIES ( Table 1 ) was validated for post-operative patients; to adapt its use for the ED, the most conservative approach is to substitute “preoperative baseline” with normal range for age.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content