
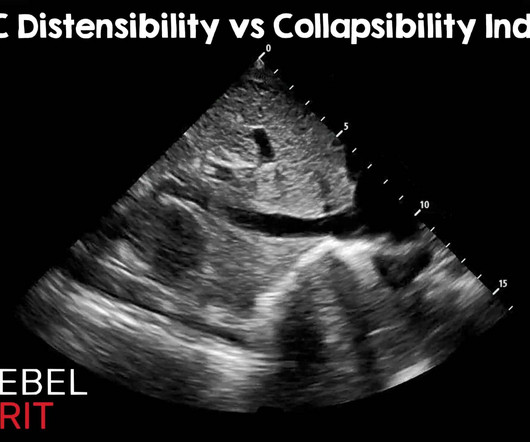
IVC Distensibility Index vs Collapsibility Index: Using the Correct Index
RebelEM
FEBRUARY 24, 2025
Of course, there are other methods of assessing fluid tolerance : Capillary refill evaluation, passive leg raise, central venous pressure measurement, pulmonary artery wedge pressures, stroke volume variation, pulse pressure variation, etc. Ultrasound Med Biol. Most measurements are somewhere around the hepatic confluence.











Let's personalize your content