This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Well keep it short, while you keep that EM brain sharp. A 73-year-old female is brought in by EMS for abdominal pain, vomiting, and weakness for two days. Operative management is necessary for signs of peritonitis, evidence of perforation, extensive bowel involvement >40cm, or after failed medical management.
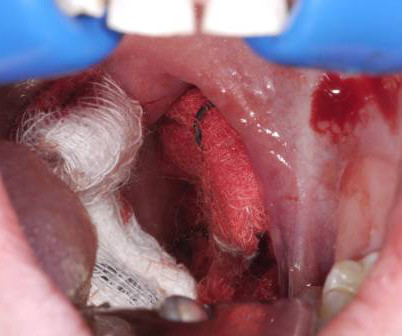
Secondary hemorrhage occurs between days five and 14 post-operatively, peaking around days five to seven. 3 A three-pronged management approach provides a framework for addressing post-tonsillectomy bleeds: resuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleeding.
We’ll keep it short, while you keep that EM brain sharp. Laborator evaluation: CBC, CMP, lipase, type and screen, coagulation panel Treatment: 1-3 Resuscitation with blood products as necessary for hemodynamic stability. A 25-year-old man presents to the ED via EMS after he sustained a gunshot wound to the left flank.
emergency medicine (EM) residency training length has been a decades-long dilemma: four vs. three years. First, is three years enough time to become an EM physician? But critical questions remain unanswered when it comes to specialization, career trajectory, and actual competence as an EM physician. 11 What should we take away?
Critically ill patients requiring resuscitation often present with many challenges including the ability to secure safe, sterile, fast, and reliable intravenous (IV) access. This can often lead to significant delays in proper resuscitation. Studies reviewed landmark-based CVC compared to IO; using IJ, subclavian, and femoral CVC sites.
A few years later, I took an active role in the EM Soc committee and helped to organise their annual conference – that year themed with a pre-hospital focus. Air Ambulance Charities operate many air ambulances in the UK and have associated rapid response cars for when the weather doesnt allow for flying.
One operator should perform defibrillation in the anterolateral position, followed by another operator providing a second shock in the anteroposterior position after a delay of less than one second. Resuscitation. Resuscitation. Resuscitation. Resuscitation. 2022;175:105-112. Sakai T, et al. N Engl J Med.
Authors: Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA), Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
Background: DKA is traditionally treated with fluid resuscitation, electrolyte replacement, and intravenous infusions of insulin. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics.
When you look for such courses, look for topics such as first aid, personal care, and resuscitation techniques. Such facilities may be fined for having problems but they remain to operate without paying penalties. This training is for nurses and those who have an administrative background whose goal is to become administrators.
pdf Equipment required for resuscitative thoracotomy: Surface anatomy: Appearance of pericardial clot A foley catheter being used to fill a cardiac wound – note how easily this could be pulled out. An open chest with aortic compression Simulation of resuscitative thoracotomy by London HEMS team. Resuscitation; 2011: 1194-1197
At REBEL EM, we’ve done an extensive write up that details some of the different types of DED and the electrophysiology behind it. Within the United States, due to paramedic shortages, this dual-medic setup does not exist in many EMS systems. This was in addition to a phenomenally fast EMS response time.
This helps relieve agitation/pain while maintaining spontaneous breathing and airway reflexes allowing for adequate pre-oxygenation as well as facilitates other resuscitation interventions including IV access, vasopressors, fluids, etc. that would not be possible in an agitated/combative patient.
emergency medicine (EM) residency training length has been a decades-long dilemma: four versus three years. First, is three years enough time to become an EM physician? But critical questions remain unanswered when it comes to specialization, career trajectory, and actual competence as an EM physician. percent versus 90.8
EMS applied combat application tourniquet to leg on scene 45 minutes ago. Intubation for clinical course and pain management need to be addressed with disposition to the operating room. No LOC but altered with some reported alcohol consumption. Was wearing a life jacket with minimal submersion.
For example, here are the locations identified as ‘2nd ICS mid clavicular line’ amongst 25 EM physicians in a 2005 EMJ paper. Pleural decompression and drainage during trauma reception and resuscitation. Journal of Special Operations Medicine : a Peer Reviewed Journal for SOF Medical Professionals , 13 (4), 53–58.
What They Did: Retrospective, observational cohort study in a single high-volume academic hospital The ED had a 5 bed area used for ongoing management and resuscitation of patients who clinically deteriorate while boarding or while actively undergo a workup in other sections of the ED. J Crit Care.
However, believers in this superstition will perceive crazier shifts if the word is uttered so you probably shouldn’t say it, or use cautiously Full moons have no impact on ED, EMS, or HEMS volumes or acuity. Nice people are not more likely to get cancer.
Rezaie, MD (Twitter: @srrezaie ) The post The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults appeared first on REBEL EM - Emergency Medicine Blog. Am J Emerg Med. 2016; PMID: 27720568 Guest Post By: Courney Knieriem, MD PGY-1, Emergency Medicine Resident RWJBH Community Medical Center, Toms River, NJ Courtneyknieriem.md@rutgers.edu
What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operating room? How can we best pick up occult cardiogenic shock before it floured shock kicks in? Which patients with acute heart are safe to send home in general?
She was reported to have had a mechanical fall, landing face forward without loss of consciousness, and has had a continuous nosebleed since then, per EMS and the home care provider. On EMS arrival, it was noted that the patient had what seemed to be a controllable nosebleed with difficulty locating the source due to constant oozing.
They may be entrapped; have limited access; may be midway in an operating position that can’t be changed; may need to be sitting due to pulmonary edema, morbid obesity, aspiration prevention or for awake intubation. Resuscitation, 56(1), 83-89. YouTube.com [Time=33’11” Presentation] EMS World. Try these situations.
It is not possible during acute resuscitation or at any time before a complete investigation, or even trial, to know who is innocent, guilty, or what occurred during the altercation. Police officers have poor hit probability, ricochets may occur, suppressive fire may be used (“keep ‘em pinned down”), or even ‘spray and pray.”
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. She was defibrillated and resuscitated.
Jeff: And while it’s not exactly core EM, we’re going to briefly discuss indications for bariatric surgery, as this is something we don’t often review even in academic training programs. Which again reiterates why this is such an important topic for us as EM clinicians to be well-versed in.
Aggressive fluid resuscitation as patients may be severely hypovolemic from GI symptoms. 5 Orogastric lavage may also be considered for GI decontamination but likely to be limited by location, size of tablets, and operator familiarity. Case Follow-up: The patient received a fluid resuscitation with 20 mL/kg bolus of normal saline.
Today, she would not get out of bed, prompting the facility to call EMS. When analyzing the receiver operating characteristic (ROC) curve of the pooled data, optimal diagnostic accuracy of MDW for sepsis prediction was seen (pooled sensitivity of 0.838 and specificity of 0.704 for Sepsis-3 criteria). She had a fever of 38.7 °C
This is the fifth part of our series on "Early Modern Resuscitation." " Part I: Oral Airways, early resuscitation, and recognition of airway care. It was not a practical resuscitative aid until production could be commercially successful (~1895) and made portable in compressed form.
In addition, a flimsy cannula is easily dislodged during ongoing resuscitation and easily clots off. This was a randomised controlled multisite study comparing resuscitation of trauma patients requiring massive transfusion using either 1:1::1 or 1:1:2 ratios of platelets to plasma to red blood cells. to −0.5%]; P = 0.03.).
r1 clinical knowledge - r4 capstone - research grand rounds - the art of em - Community corner - PEM Lecture r1 Clinical knowledge: transplant complications WITH dr. gabor Time-sensitive peri-transplant emergencies: Bleeding fistula- stop the bleed. Assessed and provided feedback of pediatric resuscitations based on video review.
Although told several times, the story of the development by Henning Ruben of the prototypical modern manual resuscitator, the self-refilling bag with unidirectional non-rebreathing valves which now dominate the world of resuscitation, is still not well-known. Czech Military resuscitation kit, 1969, mfr.
7 While post-operative adhesive disease is also a risk factor, it is far less commonly implicated in LBO compared to SBO. Measures to optimize the patient for surgical intervention and treat shock, including antibiotics and fluid resuscitation, are associated with improved outcomes in these patients.
Improved Visualization: Video laryngoscopes allow for the use of standard or hyperangulated geometry, essentially allowing the operator to “look around the corner” on an anterior airway. Operators can manipulate the blade with less force to optimize the view, making it easier to identify and navigate the endotracheal tube into the trachea.
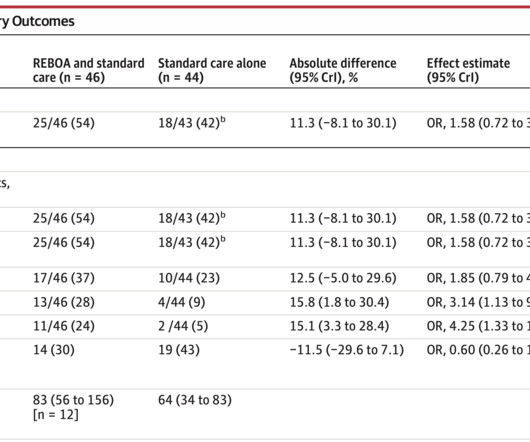
Early expeditious definitive hemorrhage control is a major focus in trauma resuscitation. Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial [published online ahead of print, 2023 Oct 12].
Resuscitative Thoracotomy in Children In a 40-year review of ED thoracotomy, Moore et al. REBOA If you have access to resuscitative endovascular balloon occlusion of the aorta or REBOA, this may be an option to temporize the child to get him to the relative control of the operating room. It is most often blunt trauma.
We should expect TXA to help in immediate stabilization and allow trauma teams the time to intervene (whether that be continued resuscitation, interventional or operative procedures). This should continue to make TXA part of standard trauma resuscitation while additional studies are performed.
Because of the retrospective nature of the study, the decision to use the bougie was operator-dependent. The effect of hand position on chest compression quality during CPR in young children: Findings from the Videography in Pediatric Resuscitation (VIPER) collaborative. Resuscitation. 2023;185:109741. O’Connell et al.
[link] The West Midlands surgical skills course offers cadaveric training for PHEM and EM practitioners on rare life saving procedures. Cricothyrotomy performed with the Melker set or the QuickTrach kit: procedure times, learning curves and operators’ preference. Click here to go straight to their page. Frerk et al. Sottile, D.,
Guest Skeptic: Dr. Rory Spiegel is a clinical instructor at University of Maryland and a recent graduate of Stony Brook’s Resuscitation Fellowship. Guest Skeptic: Dr. Rory Spiegel is a clinical instructor at University of Maryland and a recent graduate of Stony Brook’s Resuscitation Fellowship.
Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial. Methodological challenges, such as extended prehospital transport times, limited operator experience, and small sample size, introduce uncertainty to these findings.
Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial. Methodological challenges, such as extended prehospital transport times, limited operator experience, and small sample size, introduce uncertainty to these findings.
The latter 1950s and 1960s, quested for nerve gas defense studying expired air resuscitation and modern resuscitology; developing intensive care units. To me, it harkens a new scientific renaissance of resuscitation science, emergency care, and creating systems for care. 1950s & 1960s Resuscitation Research.
This post will discuss a brief overview of hospital planning and operational setup with key elements of a disaster response from events that cause high numbers of blunt trauma, penetrating trauma, burns or crush injuries that may be seen following explosive events, mass shootings, or large scale motor vehicle collisions, to name a few.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content