
Another deadly triage ECG missed, and the waiting patient leaves before being seen. What is this nearly pathognomonic ECG?
Dr. Smith's ECG Blog
JUNE 17, 2024
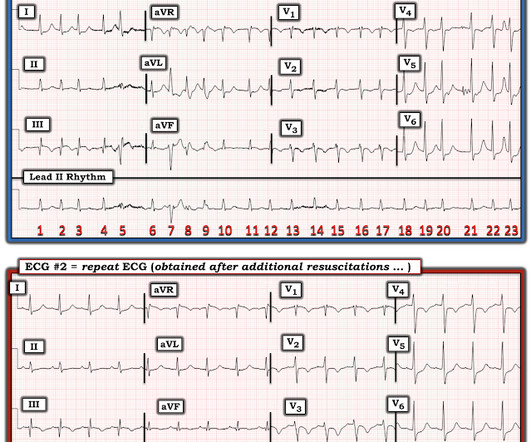
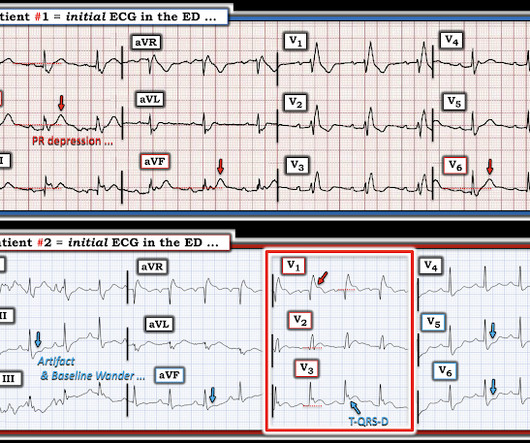
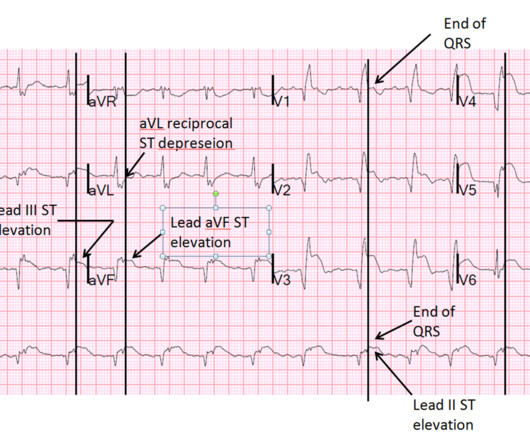
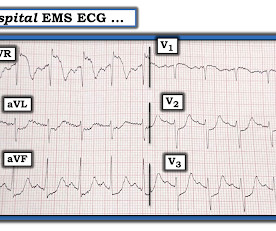
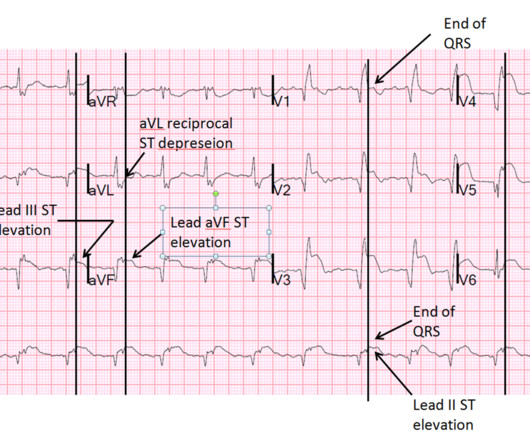
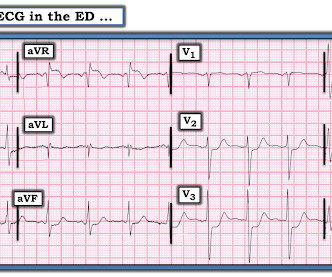
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. If this EKG were handed to you to screen from triage without any clinical information, what would you think? Do you appreciate any dynamic changes compared to the patient’s prior EKG? What do you think? In fact, Kosuge et al.





































Let's personalize your content