This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
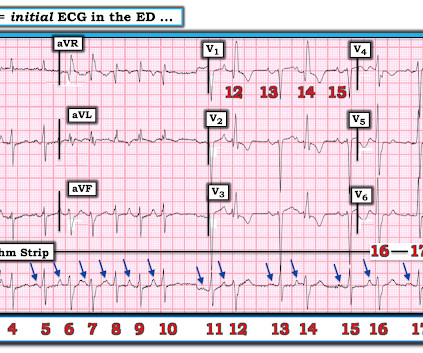
A 50-something man presented in shock with severe chest pain. His prehospital ECG was diagnostic of inferior posterior OMI. The patient was in clinical shock with a lactate of 8. Here is his ED ECG: There is bradycardia with a junctional escape. RVMI explains part of the shock. What is the atrial activity?
The STREAM-1 trial found that for [2] patients with STEMI presenting within 3 hours of symptom onset and unable to attain PCI within 1 hour of first medical contact, a pharmaco-invasive strategy resulted in similar rates of death, shock, heart failure, or reinfarction compared to primary PCI. Primary PCI: 95.7% Primary PCI: 95.7%
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Here is the initial ED ECG. Another ECG was recorded 12 minutes later: Paced rhythm, probable Pacemaker-Mediated Tachycardia ? ECG with LBBB and QRS of > 210 ms. What do you think?
However, between four and five percent of cases of VT or VF will be refractory to standard management, with nonperfusing arrhythmia persisting despite repeated shocks. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. amiodarone or lidocaine). References Tsao CW, et al.
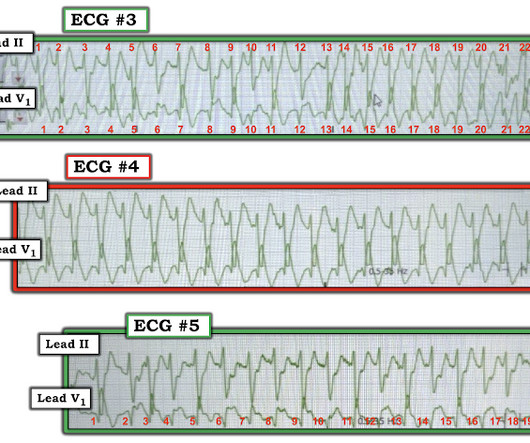
The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. How do you interpret the below ECG?
Morbidity & MOrtality - Mini Lit Blitz - Post-Rosc Care - Qi/KT Morbidity & Mortality WITH Dr. Yates Case 1: Stroke and Stroke Mimics Early diagnosis of stroke improves stroke outcomes, where misdiagnosis is associated with an upwards of 4-time higher likelihood of mortality Missed strokes most often occur with atypical symptoms, in younger (..)
Susan Wilcox Increasing regionalization due to: Growth of specialty centers Increasing development of healthcare systems Hub-and-spoke models Development of ECMO, trauma, transplant, and stroke centers The higher the acuity of the centers, the higher the acuity of the patient that needs to get there.
Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenic shock. Then I looked into the patient's chart and found an old EKG: This shows a previous QR-wave in V2, diagnostic of old anterior MI. I wrote back: "I am looking at his old EKG. Looks like atrial fibrillation.
Barometric pressure, humidity, and temperature changes may influence stroke and fall incidence (especially in elderly patients with cardiovascular risk factors). Nice people are not more likely to get cancer. Black clouds don’t exist (but I still sort of think they do).
When the physicians approached him, he was ashen, diaphoretic, and appeared in shock. When the paramedics arrived, they obtained a 12 lead ECG and confirmed the unstable vital signs. EKG is pictured below: What do you think? Why is the patient in shock? He was in profound cardiogenic shock.
Workup with a negative troponin and EKG reliably rules out BCI. Hemorrhagic shock is the most common etiology of instability in trauma and should always be highest on the differential. Posterior circulation stroke Patients with posterior strokes will likely have a low NIH. Ambulation is key during physical exam.
Here is her EKG: What is unusual about this? Here is the ECG after ibutilide: What do you notice? Here is the post-cardioversion ECG: Sinus rhythm, still with the longer QT interval. We designed a step-up protocol in which shocks at 50, 100, 200, 300, and 360 J were used for transthoracic cardioversion.
Show More v Please click here and take our listener survey Part 1: Definitions Myocardial Infarction: elevated cardiac biomarkers (aka troponin) with clinical evidence of acute myocardial ischemia (aka signs and symptoms, ECG changes, abnormal imaging, or coronary thrombosis at cath or autopsy). Diagnostics Telemetry ECG.
His ECG shows atrial fibrillation with a rapid ventricular response. SGEM#88 : Shock Through the Heart (Ottawa Aggressive Atrial Fibrillation Protocol) * SGEM#133 : Just Beat It (Atrial Fibrillation) with Diltiazem or Metoprolol? His past medical history is significant for hypertension for which he takes perindopril.
Here is the ECG: What do you think? A study of 2298 ECGs from 1085 patients which had a computerized interpretation of AF found that in 442 (19%) of these ECGs, from 382 patients (35%), the interpretation was incorrect, and that, in 92 of these 382 patients, the physician had failed to correct it. Among, 2447 ECGs, Mant et al.
Nachi: Each year, in the US, approximately 10,000 patients present with electrical burns or shocks. Pay attention to the entry and exit sites, as the pathway of the shock is predictive of the potential for myocardial injury and arrhythmia. Those with low voltage injuries and a normal EKG do not require monitoring.
Here was his prehospital ECG, which I viewed immediately while the resident performed cardiac ultrasound: What do you think? Here is the cardiac ultrasound which the resident performed as I viewed the ECG: This shows a huge pericardial effusion. An ED ECG was recorded: What do you think? Fluids were started. Is is sinus?
stent, percutaneous nephrostomy) by urology or IR Hypokalemia evaluate for EKG changes assess for underlying cause and factors that may influence ability to replete (i.e. Vaishnav Hyperthermia: abnormally high body temperature due to thermoregulatory failure Severe hyperthermia: temp greater than 40.5C
Exertional Hyperthermia Patients with heat stroke will present with Temp > 104, AMS, or seizures. EMS was bagging him on arrival Primary notable for Compromised Airway Protection, bilateral Breath sounds, strong pulses,GCS 3 CT images of Head, Chest, Abdomen, Pelvis, and Spine No acute findings pH of 6.75
Electrocardiography (ECG) should be performed on any patient with significant blunt chest injury. A negative ECG is highly consistent with no significant blunt myocardial injury. Any patient with a new abnormality on ECG (dysrhythmia, heart block, or signs of ischemia) should be admitted for continuous ECG monitoring.
Jeff: There are a shocking 22 million past-month users of marijuana in the US, followed by pain relievers at 3.8 First up is the link between cannabis use and stroke or TIA. times higher risk of stroke or TIA. Jeff: For any patient arriving with suspected cannabis or synthetic abuse, consider checking an EKG.
A 12-lead EKG shows sinus tachycardia but is otherwise normal. Both can result in heat exhaustion and heat stroke and have many overlapping symptoms. Patients with heat stroke have hot, dry skin and altered mental status (e.g., C, and heat stroke occurs at a core temperature > 40°C. Temps greater than 41.5C
After initiation of stroke prevention regimens—often with oral anticoagulation.) The first primary endpoint was a composite of CV death, stroke, hospitalization for heart failure or acute coronary syndrome. They transmitted single-lead ECGs twice per week or when symptomatic. Stroke was even lower at 0.6%
A repeat bedside ECG showed complete resolution of tamponade findings (Figure 2), no appreciable pericardial effusion, and relocation of the heart to typical anatomic location. Figure 2. (A) In normal physiology, inspiration leads to increased negative intrathoracic pressure, allowing for increased preload of both ventricles.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content