This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
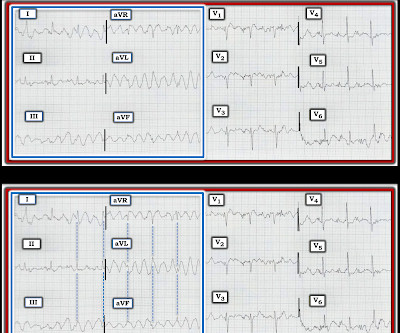
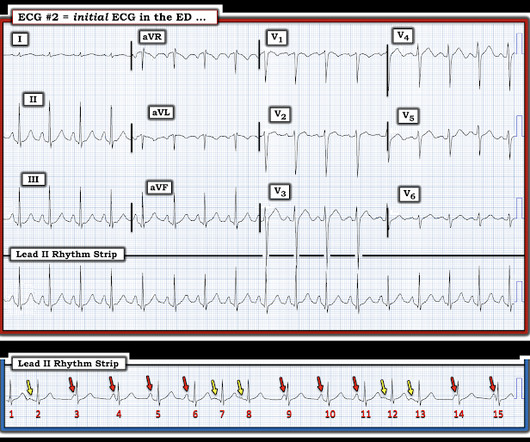
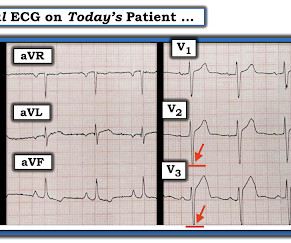
I was sent the ECG in Figure-1 — without the benefit of any history. Figure-1: I was sent this ECG without any history. MY Thoughts on Today’s CASE: As tempting as it might be to reach for the defibrillator on seeing the ECG shown in Figure-1 — My initial reaction was different. Is this VT? Is this VT? What to do next ?
1 Seizures may occur due to lowered seizure threshold. 6 Seizures have been observed and are dose-dependent. Recommend obtaining multiple EKGs to aid in the diagnosis of cardiotoxic effects such as dysrhythmias or interval widening, even if not apparent immediately after the overdose. 8 Hypersalivation can occur.
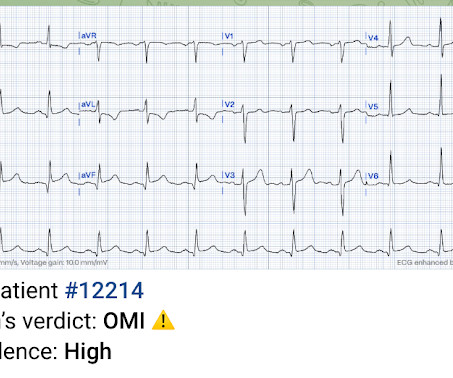
This 60 yo male had an apparent tonic clonic seizure. He had no history of seizures. He had a prehospital ECG: What do you think? But syncope or seizure alone, without chest pain, is not enough to call it Wellens syndrome. So she will call Wellens' ECG "OMI". So she will call a Wellens' ECG "OMI".
Emergency medical services (EMS) were called to the home of a 22-year-old woman after a syncopal episode and seizure-like activity. She was transported to the emergency department, and the following ECG was obtained (Figure1). The post <i>Annals</i> ECG of The Month appeared first on ACEP Now.
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Check glucose, obtain imaging, stop the seizure. They administer two doses of 10 mg midazolam IM.
He had a prehospital ECG. They recorded a prehospital ECG: What do you think? The Queen of Hearts interprets it blinded also (no clinical information and no previous ECGs or serial ECGs). And that is what we see in the presenting 2 ECGs at the top. A 50-something had syncope while driving. Learning Points: 1.
A young man presented after a prolonged seizure. Here was his initial ECG: Regular Wide Complex Tachycardia. Here is the same ECG with some annotation (lines): The first line is drawn at the onset of the QRS in V2, which is clear. Here is the subsequent ECG: This is clearly sinus tach. The patient was unconscious.
REBEL Core Cast 109.0 – Na Channel Blocker Poisoning Click here for Direct Download of the Podcast Definition and Physiology Standard definition of a wide QRS is anything > 120 msec (3 small boxes on the ECG) In the context of poisoning, a “wide QRS” is anything greater than 100 milliseconds. Boehnert 1985 ). N Engl J Med.
We cover GRACE-1, communicating stats better, managing seizures after initial control, POCUS for intussusception, and reading STEMI on ECG with a paced rhythm. It’s the JournalFeed Podcast for the week of August 2-6, 2021.
The ECG below is taken from an 83 year old man with a seizure history for the past 8 years. He presents after two 10 minute generalised tonic-conic seizures at home 10 days after self ceasing his C…
The ECG below is taken from an 83 year old man with a seizure history for the past 8 years. He presents after two 10 minute generalised tonic-conic seizures at home 10 days after self ceasing his C…
Avoid routine seizure prophylaxis in adult survivors of cardiac arrest (Level 3: no benefit), but treat seizures if they occur (Level 1: strong). Editorial Comment : Yes to PCI after arrest with STEMI on ECG. Treatment of nonconvulsive seizures (diagnosed by EEG only) is reasonable in adult survivors of cardiac arrest.
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. EEG Monitoring and Seizures Statements Takeaway: If possible, obtain an EEG to evaluate for seizure activity.
Here is the ECG: The computer reads a long QT at 449 ms, and a Hodges QTc of 506 ms. This was the etiology of seizures. From EMCrit: Taking control of severe hyponatremia with DDAVP An ECG recorded 2 days later with a K of 4.1: Figure-1: Both ECGs that were done in this case ( See text ). What do you think?
She reportedly received a landmark guided peripheral nerve block with bupivacaine and shortly thereafter developed generalized seizures. 1,5] CNS symptoms include: Seizure, coma, altered mental status. [1] 1-3,5,7,9] All patients developing symptoms of LAST should be placed on a continuous cardiac monitor and have an ECG performed. [2]
Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). As I discuss in detail in My Comment at the bottom of the page in the May 24, 2020 post in Dr. Smith's ECG Blog — AV dissociation is not the same as AV block. How would YOU interpret this tracing?
This patient presented with weakness, decreased urine output, and vomiting: What is the ECG diagnosis? Here was a repeat ECG: QTc 523. The value of recognizing this particular ECG pattern — is that it may expedite your clinical diagnosis even before laboratory results return. This is pathognomonic for hypocalcemia.
The minute this medical student saw the first ECG, he knew the diagnosis without any further information. Reading ECGs is hard, but can be done with commitment to learning, which comes from an awareness of its importance. You need to be interested and understand the value of the ECG. She had this ECG recorded: ECG 1: QTc is 484.
A 64 year old male presents to ED after multiple seizure episodes that day. It was reported that the patient would have 20 seconds of seizure activity and then make a full recovering. The patient h…
The preshospital ECG and strips are not available. Here is the first ED ECG: What is the likely diagnosis? There is sinus tachycardia, a prolonged QRS (computer read it as 114 ms, previous ECG with 102 ms). Of 14 with initial QRS of 140 ms or longer, 8 (56%) had seizures. There is a large R-wave in lead aVR.
You have been handed over a 58 year old male patient who presented yesterday with a seizure on a background history of alcohol dependence. He also has a history of depression and GORD. He has never…
You have been handed over a 58 year old male patient who presented yesterday with a seizure on a background history of alcohol dependence. He also has a history of depression and GORD. He has never…
morbidity and mortality - quality improvement - research grand rounds - r1 clinical knowledge: pres/rcvs - r4 case follow-up: compartment syndrome Morbidity and Mortality WITH dr. finney Takotsubo Cardiomyopathy with COVID-19 Increasing incidence of Takotsubo Cardiomyopathy with the COVID-19 pandemic Morbidity and mortality is similar to that of ACS (..)
Cardiac Differentiating syncope from seizure Features that point to seizure Urinary incontinence Number of jerks Age? Glucose ECG ED History - table 4 History of similar Prodrome Associated symptoms (chest pain, neuro symptoms, etc) Falls Pre-syncope ? ECG Brugada, blocks, VT, ST changes, etc Labs BNP, delta bnp ?
David Carr joins Anton to give us his simplified approach to syncope based solely on history, physical and ECG to help guide disposition decisions. We answer questions such as: What features have the best likelihood ratios to help distinguish syncope from seizure?
At 3:55 AM during that kind of a night shift, this ECG (among many others) was brought from triage for review by my team. We knew only that the ECG belonged to a man in his 50s with chest pain and normal vitals. Here is the computer interpretation: So we have a triage-computer-normal ECG. No prior available.
A 64 year old male presents to ED after multiple seizure episodes that day. It was reported that the patient would have 20 seconds of seizure activity and then make a full recovering. The patient h…
Then I looked into the patient's chart and found an old EKG: This shows a previous QR-wave in V2, diagnostic of old anterior MI. I wrote back: "I am looking at his old EKG. The cath lab had been activated and then they sent me the ECG. They agreed that the ECG findings were due only to old MI and tachycardia.
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. These systemic effects can include central nervous system (agitation, seizures , and coma), as well as cardiac ( hypotension and dysrhythmias) [10, 11]. Administer high-flow oxygen if indicated and consider arterial blood gas ( ABG ).
If you or your patient do not have a watch capable of providing you with an ECG, consider asking those on board to allow you to borrow theirs. Get a blood gas when possible to help guide your ventilation. Some newer AED's have the capability of providing you with a rhythm strip.
Before EMS arrived, she had "seizure activity" and became unresponsive. She arrived comatose and in cardiogenic shock and the following ECG was recorded. A 56 yo f with h/o HTN and hypercholesterolemia called EMS from home after onset of L chest pain radiating to the left arm. She was intubated. She was bradycardic and hypotensive.
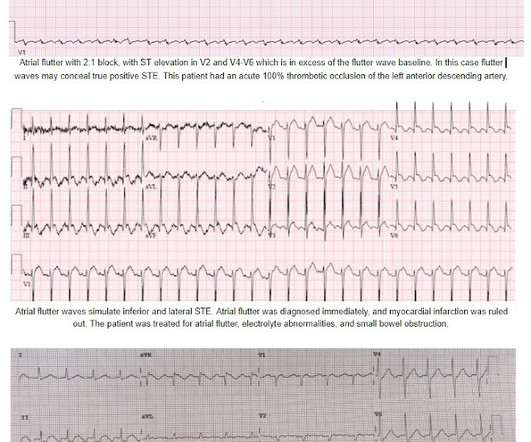
Side note: The differential of sudden persistent loss of consciousness with adequate hemodynamics is relatively short: seizure, intracranial hemorrhage, basilar artery occlusion. An ECG was recorded quickly on return to the ED: (sorry for poor quality, cannot get originals) What do you think? Atrial flutter was recognized at this time.
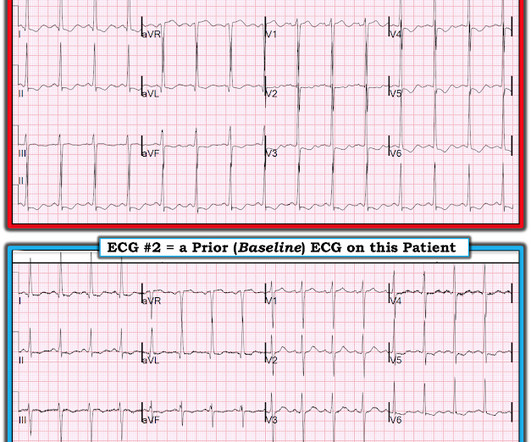
He had a seizure this morning and rolled out of bed unable to get up. The medics recorded a prehospital ECG: The computerized QTc is 397 ms Jason writes: " What's your thoughts Steve?" Unfortunately, the R-wave is cut off on this ECG but it appears as if it would be at least 20 mm. So this was the patient's baseline ECG.
He had a seizure this morning and rolled out of bed unable to get up. The medics recorded a prehospital ECG: The computerized QTc is 397 ms Jason writes: " What's your thoughts Steve?" Unfortunately, the R-wave is cut off on this ECG but it appears as if it would be at least 20 mm. So this was the patient's baseline ECG.
This was sent by a recent ultrasound fellow, asking for my ECG diagnosis. These ECGs, in my experience, are not seen in ACS. This patient presented with altered mental status and seizure, so the diagnosis of Takotsubo can be made without angiography or even echo. There is ST elevation in I, II, III, aVF, V2, V3, V4, V5, and V6.
mepivacaine (1-3 h) 1% lidocaine +/- epi (2-3h) 0.25% bupivacaine (2-3 h) 0.25-0.5% mg/kg IV Versed: 0.2 mg/kg IM, 0.2 mg/kg IN (may repeat to max of 0.4 mg/kg IN), 0.2 mg/kg IV Versed: 0.2 mg/kg IM, 0.2 mg/kg IN (may repeat to max of 0.4 mg/kg IN), 0.2 mg/kg IV Versed: 0.2 mg/kg IM, 0.2 mg/kg IN (may repeat to max of 0.4 mg/kg IN), 0.2
Patient C, a 27-year-old female with a history of epilepsy, taking valproate and endorsing adherence, is then brought in by ambulance for a witnessed seizure. This is her first seizure in six years. This patient had her first seizure in years despite adherence to her valproate for management of her epilepsy.
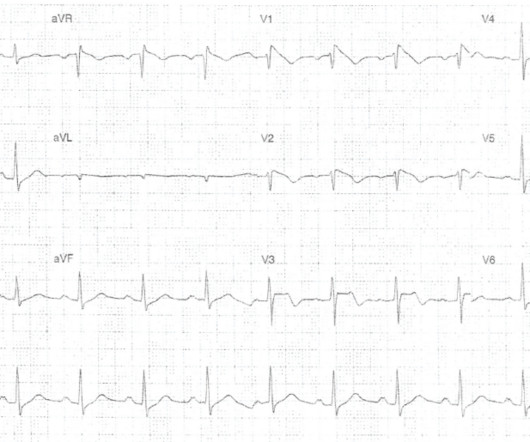
This ECG was recorded on a middle-aged male with sickle cell disease and diffuse pain. Here is a Previous ECG for comparison: Baseline LVH Only minimal ST depression Diffuse ST depression with ST Elevation in aVR Knotts et al. Any hypokalemia that results in clear ECG abnormalities, such as here. What do you think?
Some important causes to consider include reflux (very common), seizures, and maltreatment/NAI. Other tests: At most, guidelines suggest that an ECG and pertussis test may be undertaken. An event cannot be said to be unexplained unless you have tried to explain it.
1 , 2 The most common non-iatrogenic cause is spontaneously due to increased intraesophageal pressure, Boerhaave syndrome, from forceful retching, coughing, straining, seizures, or even childbirth (15% of cases). upper endoscopy, transesophageal echo, etc.). Abdomen: Evidence of peritonitis if intra-abdominal rupture.
stent, percutaneous nephrostomy) by urology or IR Hypokalemia evaluate for EKG changes assess for underlying cause and factors that may influence ability to replete (i.e. EtOH, amphetamines, or cocaine) Prescription drugs (i.e.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content