
Resuscitated from ventricular fibrillation. Should the cath lab be activated?
Dr. Smith's ECG Blog
JULY 25, 2024
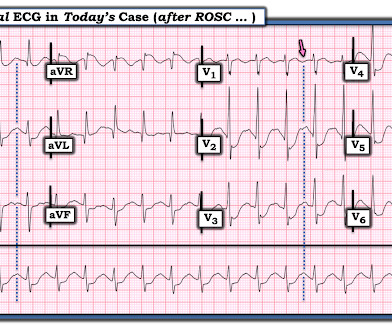
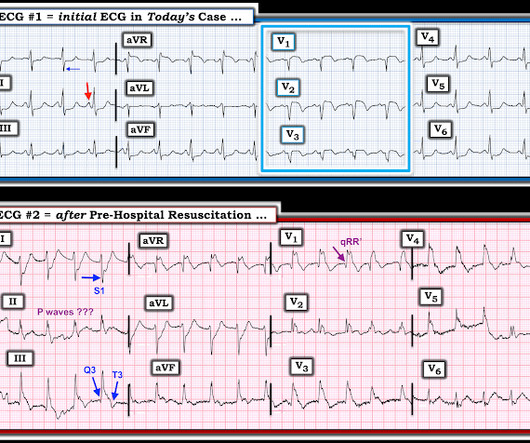
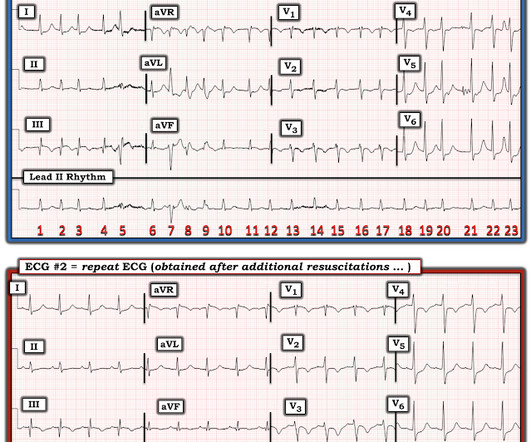
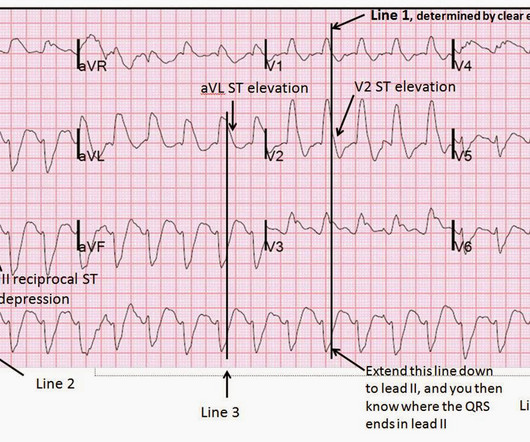
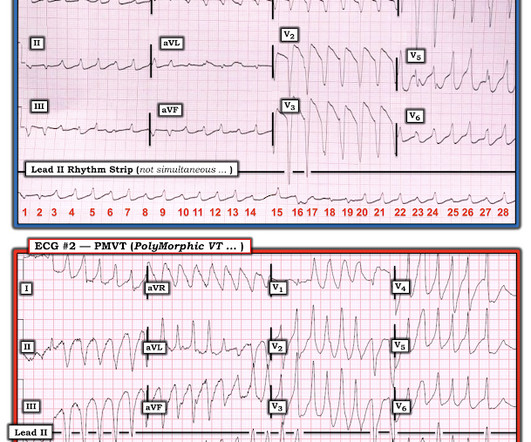
The patient was brought to the ED and had this ECG recorded: What do you think? The ECG shows severe ischemia, possibly posterior OMI. After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another. == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process.





































Let's personalize your content