

ECG Blog #394 — Is QRS Morphology Disguised?
Ken Grauer, MD
SEPTEMBER 8, 2023
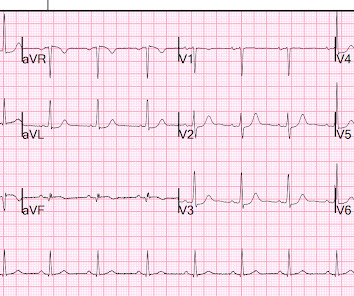
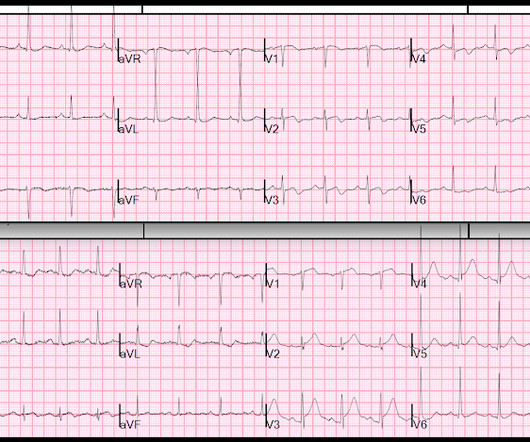
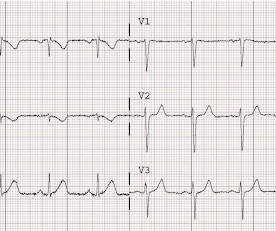
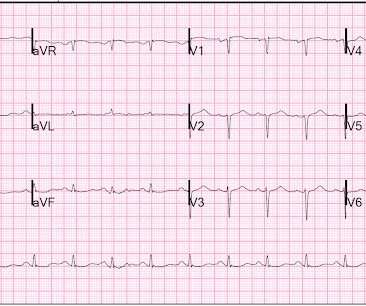
The ECG in Figure-1 — was obtained from an older man with a history of prior infarction and coronary bypass surgery. Figure-1: The ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). There is no ECG indication of chamber enlargement — ST-T wave changes do not look acute.





































Let's personalize your content