

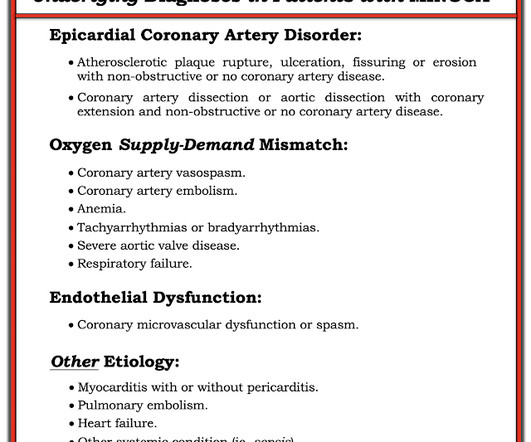
Chest pain, resolved. Does it need emergent cath lab activation (some controversy here)? And much much more.
Dr. Smith's ECG Blog
APRIL 22, 2024
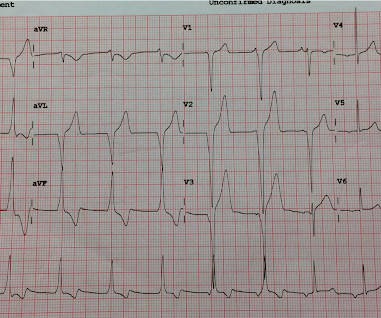
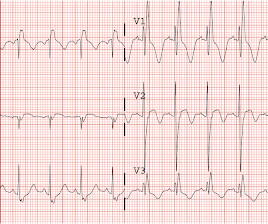
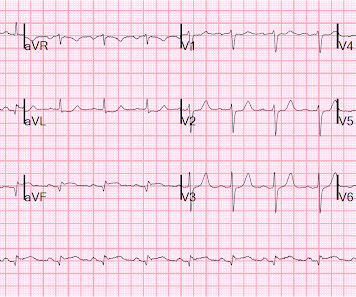
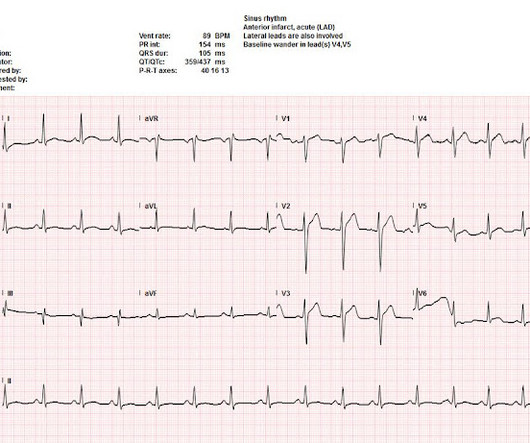
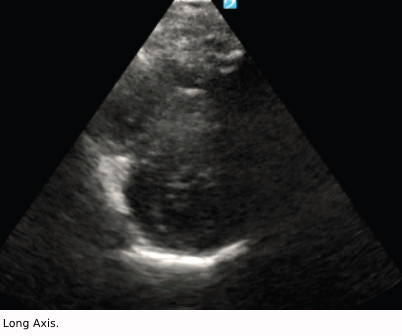
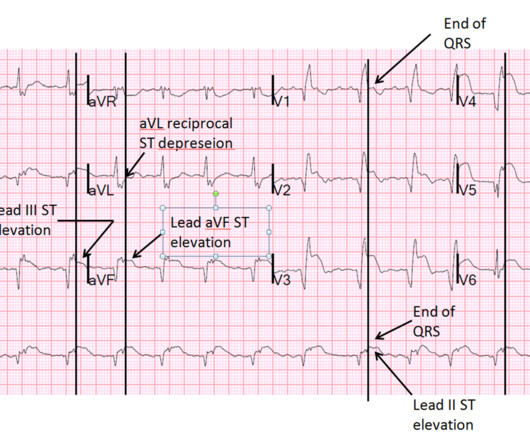
EKG from triage: Here is his previous ECG: Normal ST Elevation Resident's interpretation: Reperfusion pattern/Wellens' with biphasic T waves in V2 and V3, and in comparison to an EKG in 2020 this is new. Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain.





































Let's personalize your content