This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Recommend obtaining multiple EKGs to aid in the diagnosis of cardiotoxic effects such as dysrhythmias or interval widening, even if not apparent immediately after the overdose. 1,2 Cardiovascular: Obtain an initial EKG to determine the patient’s baseline and repeat. J Emerg Crit Care Med Vol 6 (October 30, 2022) J Emerg Crit Care Med.
The ECG below was recorded about 20 minutes after he regained consciousness. ECG #1 The above ECG shows sinus rhythm at about 60 bpm. Figure A It now becomes apparent that there is ST segment depression in almost every lead of the ECG (V1-V6, I, II, aVL and aVF). In the initial ECG (ECG# 1) aVR had ST elevation.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. An initial electrocardiogram (ECG) is provided below. A subsequent ECG was taken: There is persistent ST elevation, especially being concordant in inferolateral leads.
His initial EKG is the following: What do you think? Do we still shock? Its narrow indication for stable VT means many emergencydepartments may not routinely stock the medication. If procainamide is utilized, a baseline EKG should be obtained to assess the QRS and QTc at baseline. Are there any meds you can give?
Authors: Adam Roussas, MD, MBA, MSE // Reviewed by: Jamie Santistevan, MD ( @jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD ( @MPrizzleER ); and Brit Long, MD ( @long_brit ) Case A 40-year-old female presents to the emergencydepartment for palpitations and lightheadedness. What do you do?
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergencydepartment, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
The photos that Dr. Clarke took from 19781980 provide a glimpse into working in an emergencydepartment in the years the specialty was being established. Medical anti-shock trousers (MAST) being applied for a trauma patient and a Datascope cardiac monitor in use during traumatic full arrest. Click to enlarge.) Click to enlarge.)
89% agree that violence in the emergencydepartment has harmed patient care. Scrutinize but don’t overthink (interpret your EKGs with context) Know your splints Be comfortable with OMI EKGs Know your resources & know when to ask for help Be creative
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. These diagnoses were not found in his medical records nor even a baseline ECG. The patient continued having chest pain.
He had the following EKG recorded: Low voltage, suggests effusion. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. Assessment was severe sudden cardiogenic shock. He remained hypotensive and in shock. He was moderately hypoxic.
Glucose POC ECG: Is this actually sinus tachycardia? Looking at the initial or even repeating the ECG will be helpful here. Additional resuscitation Have we addressed all potential sources of shock for the patient in front of us? Does the patient require blood, a procedure to address obstructive shock, or other source control?
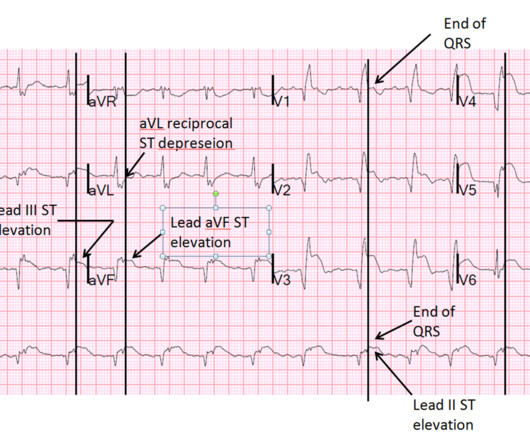
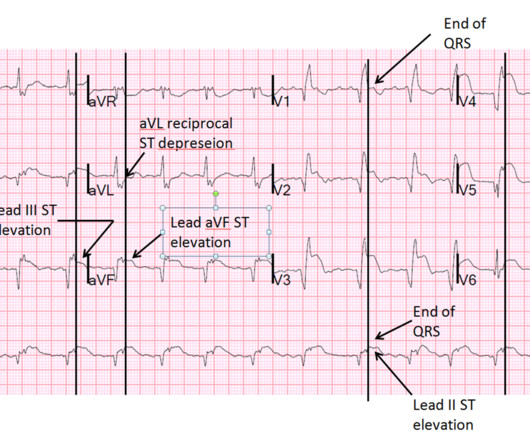
He presented to the EmergencyDepartment with a blood pressure of 111/66 and a pulse of 117. He had this ECG recorded. He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6.
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 6 What Can I Do Outside of Repeated Shocks and Standard ACLS? Circulation.
This month, after a few months of primarily medical topics, we’re talking trauma, specifically Blunt Cardiac Injury: EmergencyDepartment Diagnosis and Management. Consider valvular injury in any patient who appears to be in cardiogenic shock, has hypotension without obvious hemorrhage, or has pulmonary edema.
She presented to the emergencydepartment after a couple of days of chest discomfort. The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. How do you interpret the below ECG? This is very prolonged.
Colin is an emergency medicine resident beginning his critical care fellowship in the summer with a strong interest in the role of ECG in critical care and OMI. A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergencydepartment with 5 days of “flu-like” illness.
But this month’s episode is special in its own way - we’ll be tackling Electrical Injuries in the emergencydepartment - from low and high voltage injuries to the more extreme and rare lightning related injuries. Nachi: Each year, in the US, approximately 10,000 patients present with electrical burns or shocks. That’s -- high.
Show Notes Please click here and take our listener survey EmergencyDepartment management of Non-St Segment Elevation Myocardial Infarction, by Drs Julianna Jung and Sharon Bord. MACE= Major Adverse Cardiovascular Event: including re-infarction, stroke, dysrhythmia, heart failure, cardiogenic shock, and death.
She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. The EKG shows sinus tachycardia with nonspecific changes and no ST segment elevations, Q waves, or hyperacute T waves. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
In this episode, Sam Ashoo, MD interviews Adam Sigal, MD and Stephanie Costa, MD - the authors of the August 2022 EMP article on Managing Acute Cardiac Valvular Emergencies in the EmergencyDepartment. Listen to the discussion to hear more about the emergency medicine approach to valvular emergencies.
Table 3 ADD-RS score Exam Diagnostics Labs EKG – STEMI? Imaging CXR Echo CT MRI Aortogram Treatment BP management Heart Rate Shock Surgery – Who goes and when? It is in Beta and your feedback is welcome. Risk Factors Prehospital Care – what should EMS be looking for? ED Care History HTN, Pulse defecits, Chest Pain, Syncope?Table
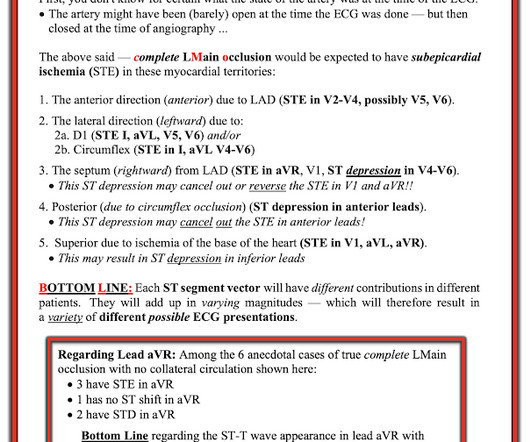
Some total LAD occlusion manifest on the ECG similarly to some left main occlusions. Depending on where the STE vector of the LM occlusion shows up on the ECG, there may be either STE, or STD, or neither in aVR, and lead aVR will not be the important part of the ECG interpretation in these cases.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. ng/mL (ULN 0.04).
Statistically, 1/10 patients who present to the emergencydepartment have hepatitis C, with an estimated 2.5-3.5 Diaz, Fabiano, And martella The presentation of adrenal crisis is often nonspecific, so it is important to keep a broad differential in cases of undifferentiated shock. and Kathleen Hildreth, Pharm.
Think about ECG as an example, So, where the box is green, the test has given us the correct result for the patient. Am J Emerg Med. One year mortality of patients treated with an emergencydepartment based early goal directed therapy protocol for severe sepsis and septic shock: a before and after study.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. It is true this ECG does not meet STEMI criteria (there is 1.0
Yates Case 1: Stroke and Stroke Mimics Early diagnosis of stroke improves stroke outcomes, where misdiagnosis is associated with an upwards of 4-time higher likelihood of mortality Missed strokes most often occur with atypical symptoms, in younger aged patients, those with posterior strokes, and those with lower NIH scores It can be difficult to discern (..)
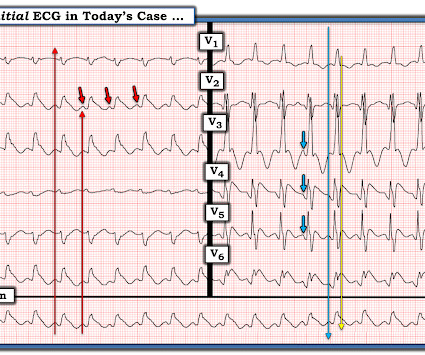
What is your ECG interpretation and what would you do next? This ECG shows a normal sinus rhythm with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, late R wave progression (and misplaced V2), normal voltages, ST-elevation in aVR and global ST-depressions. BP was 110 and oxygen saturation was normal.
This month, we are sticking in the abdomen for another round of evidence-based medicine, focusing on EmergencyDepartment Management of Patients With Complications of Bariatric Surgery. Consider performing a RUSH exam (that is rapid ultrasound for shock and hypotension) to identify the cause.
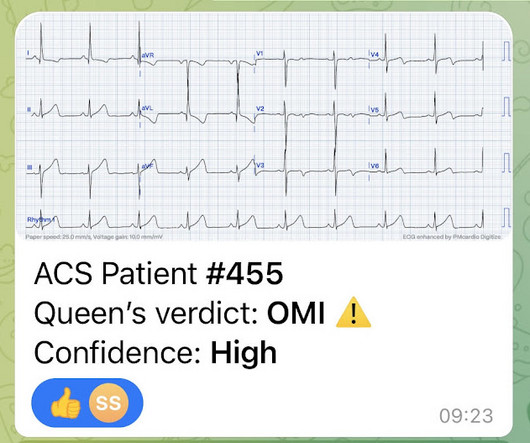
ECG PATTERN RECOGNITION CARDIAC ARREST AND ST ELEVATION: [BLOG]: Dr. Smith features a brief cardiac arrest case with an ECG pattern that you must know and be able to recognize! BONUS: User this article to identify what type of device your patient has if in the rare circumstance they don't know. Check out his post here.
Case: A 55-year-old male presents to the emergencydepartment with sudden onset of palpitations and pre-syncope starting one hour ago. His ECG shows atrial fibrillation with a rapid ventricular response. His ECG shows atrial fibrillation with a rapid ventricular response. Reference: Scheuermeyer et al.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. Electrical injuries—excluding lightning injuries—account for roughly 10,000 nonfatal shock incidents a year and 500 deaths a year.
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). In this case, profound shock for 1 hour would result in the same degree of infarction. A followup ECG was recorded 2 days later: No definite evidence of infarction. Did YOU see them?
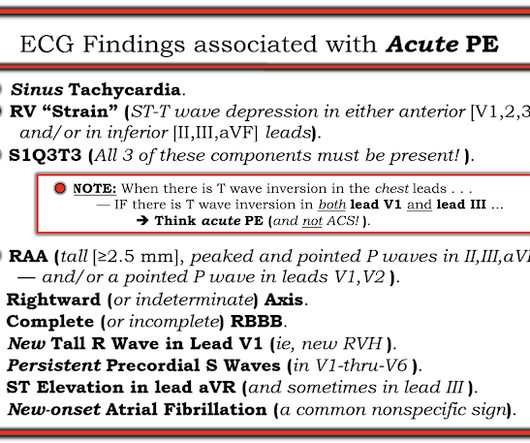
4 In an emergencydepartment (ED) presentation of cardiac arrest, the diagnosis of PE is challenging without the use of CT angiography. Point-of-Care-Ultrasound (POCUS) is a bedside modality that can assist Emergency Physicians (EPs) in differentiating PE from other causes of cardiac arrest. EKG RV strain.
Here is his ECG: What is your interpretation? Case Continued 2 days later the patient became increasingly tachycardic, hypotensive, ashen, clammy (in cardiogenic shock) and had a new murmur. This was the 12-lead ECG. This remains consistent with PIRP, as was the first ECG. Ann Emerg Med 1994; 23(6):1333-42.
Written by: Elizabeth Stulpin, MD (NUEM ‘23) Edited by: Aaron Wibberly, MD (NUEM ‘22) Expert Commentary by : Joshua Zimmerman, MD (NUEM ‘17) Non-Response to Vasopressors Shock is defined as a state of cellular and tissue hypoxia resulting in end organ dysfunction. And for most forms, EM physicians are not typically shocked by shock.
Here is his ECG: There is atrial fibrillation at a rate of 95. Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock. This was the 12-lead ECG. This remains consistent with PIRP, as was the first ECG.
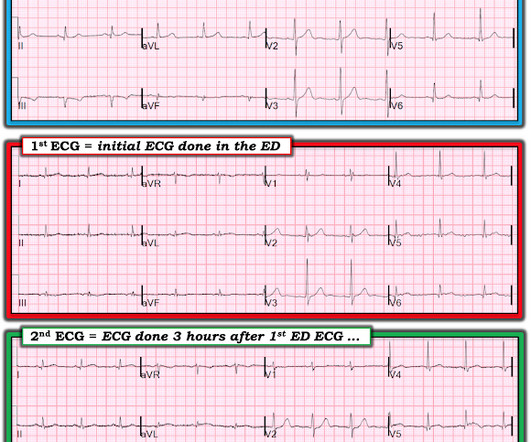
He had a triage ECG at time 0 (ECG-1): Computer read, with Physician overread: Sinus rhythm. If you see this, you must very closely question the patient about any chest symptoms, and even if no relevant symptoms, to be certain to look for old ECG, and to do serial ECGs and troponins. A 3rd ECG was recorded at 3.5
She had just left the hospital, and had so many scheduled doctor’s appointments over the next several weeks that the last thing she wanted to do was going to the emergencydepartment. The ECG shows a bradycardia at rate of approximately 36 bpm. There were things to do around the house…shopping, cleaning, mail.
Acute management of atrial fibrillation in congestive heart failure with reduced ejection fraction in the emergencydepartment. Acute management of atrial fibrillation in congestive heart failure with reduced ejection fraction in the emergencydepartment. Date: January 4th, 2023 Reference: Hasbrouck et al.
A retrospective evaluation of phenobarbital versus benzodiazepines for the treatment of alcohol withdrawal in a regional Canadian emergencydepartment Link: [link] Bottom Line: This study in a small regional ED showed a QI project rolling out a Phenobarbital or Diazepam for Alchohol withdrawal syndrome. and NPV(50%).
It’s a high-flow artery to the face, and if disrupted, the child may have significant bleeding and possibly hemorrhagic shock. Regardless of the exposure, obtain an ECG and look for bundle branch block, heart block, and dysrhythmias , since those will change disposition. J Emerg Med. Electrical Injuries: Shocking or Subtle?”
stent, percutaneous nephrostomy) by urology or IR Hypokalemia evaluate for EKG changes assess for underlying cause and factors that may influence ability to replete (i.e. EtOH, amphetamines, or cocaine) Prescription drugs (i.e.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content