This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 36-year-old male presents to the emergencydepartment after being found down at home by his spouse. Upon EMS arrival the male is noted to be anxious and tremulous with a GCS of 14. Acad Emerg Med. This series provides evidence-based updates to previous posts so you can stay current with what you need to know.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Recommend obtaining multiple EKGs to aid in the diagnosis of cardiotoxic effects such as dysrhythmias or interval widening, even if not apparent immediately after the overdose. 1,2 Cardiovascular: Obtain an initial EKG to determine the patient’s baseline and repeat. His roommate found an empty pill bottle on the floor next to him.
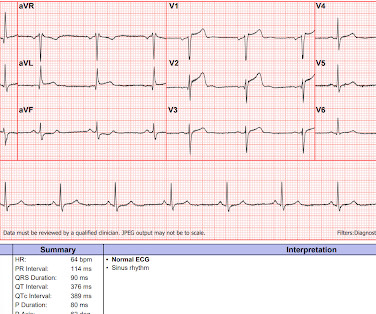
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Emergency medical services (EMS) were called to the home of a 22-year-old woman after a syncopal episode and seizure-like activity. On EMS arrival, the patient was alert, pulse was fluctuating between 40 and 130 beats/min, and manual systolic blood pressure was 60 mmHg.
These are commonly encountered in the emergencydepartment, so being able to correctly identify the rhythm is extremely important. When you are presented with a tachycardic ECG, there are two major factors we want you to focus on right away. This ECG comes from a 22-year-old female presenting with palpitations.
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergencydepartment with shortness of breath or chest pain. The post ECG Cases 49 – ECG and POCUS for Dyspnea and Chest Pain appeared first on Emergency Medicine Cases.
We’ll keep it short, while you keep that EM brain sharp. Her presenting EKG is shown below. Clinical features Patients often present after an episode of sudden syncope, although Brugada syndrome can also be found on a routine EKG. ECG to evaluate for arrhythmia. Neurological exam is also unremarkable.
These are very commonly encountered in the emergencydepartment, so being able to correctly identify the rhythm is extremely important. When you are presented with a tachycardic ECG, we want you to focus on two major factors right away. This ECG comes from a 75-year-old female presenting with palpitations. Let’s dive in!
We’ll keep it short, while you keep that EM brain sharp. A 74-year-old female with a past medical history of hypertension, diabetes, recent basilar artery stent placement with a 20 pack-year smoking history presents to the ED via EMS for altered mental status and episodes of apnea. Ann Emerg Med. Erratum in: Ann Emerg Med.
Written by Pendell Meyers A teenager was involved in a motor vehicle collision and presented to the EmergencyDepartment via EMS altered and potentially critically ill. Here is his initial ECG around 1330: What do you think? Troponins and EKGs should be trended until normalization (Sybrandy).
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. With EMS, patient had a GCS of 3 and was saturating 60% on room air. Vital signs were within normal limits on arrival to the EmergencyDepartment. or basilar ischemia.
As we all know, a critical concern for emergency physicians is identifying patients with heart tissue-threatening ischemia that could benefit from percutaneous catheterization via stent deployment by an interventional cardiologist. The chosen vernacular for these ECG findings has been traditionally called “STEMI equivalents”.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. What do you think of the ECG, and does it matter? But does this matter? But only 6.4%
She was brought to an EmergencyDepartment for evaluation. Here is her ECG: What do you think? This ECG shows sinus bradycardia with massively long QT (or QU?) She then had several more syncopal episodes the next day, and returned to a different EmergencyDepartment. The patient was sent home!
Authors: Adam Roussas, MD, MBA, MSE // Reviewed by: Jamie Santistevan, MD ( @jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD ( @MPrizzleER ); and Brit Long, MD ( @long_brit ) Case A 40-year-old female presents to the emergencydepartment for palpitations and lightheadedness.
His initial EKG is the following: What do you think? Its narrow indication for stable VT means many emergencydepartments may not routinely stock the medication. If procainamide is utilized, a baseline EKG should be obtained to assess the QRS and QTc at baseline.
The Patient This ECG is from a 57-year-old man complaining of sub-sternal chest pain for 30 minutes. EMS found him pale, diaphoretic, and anxious. The ECG The rhythm is normal sinus rhythm at 98 bpm. but rather a STEMI equivalent, warranting emergent treatment in a cath lab.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. No troponins were measured! Long term follow up is unavailable.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the EmergencyDepartment via ambulance for respiratory distress and tachycardia. Here is the prehospital ECG: First ED ECG What do you think?
The specialty, he said, spoke to his interest in surgery and EMS in a way that family medicine did not. A phone call to LA CountyUSC revealed that the emergency medicine program had one spot left for the following year. Emergency medicine was fairly new then, and most attendings were not emergency physicians, Dr. Clarke said.
EMS arrived and recorded this ECG: What do you think? See same ECG below with computer automated interpretation, using the Glasgow ECG algorithm which apparently is used by many different providers and devices Amazing that the computer calls this normal. Next day ECG. And yet it still says "normal".
Date: February 28, 2024 Guest Skeptic: Dr. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. He is the Vice Chair of the EmergencyDepartment at Nassau University Medical Center in East Meadow, NY, the safety net hospital for Nassau County. AEM February 2024.
EKG, labs, and a CXR are interpreted by the EP as normal. An attorney is consulted and a lawsuit filed against the hospital, the first ED physician, the EM group, and the PCP. Too much weight was given to the EKG, CXR, and labs. Plaintiff : You told me you would call me if the radiology report was “different.” Baccei SJ et al.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. These diagnoses were not found in his medical records nor even a baseline ECG. The patient continued having chest pain.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Smith comment: Go here for a comprehensive blog post on syncope and link to the most detailed version of the Canadian Syncope Rule: EmergencyDepartment Syncope Workup. Troponins were all negative.
Episode 67 – Managing Postpartum Complications in the EmergencyDepartment – An Interview with Dr. Nicole Yuzuk, Dr. Joseph Bove, and Dr. Riddhi Desai EMplify – March 2022 Interview with the Authors: Nicole Yuzuk, DO, Joseph Bove, DO, and Riddhi Desai, DO Episode Outline: 1.Why Why is this an important topic in EM?
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Our first 12 lead ECG was then recorded at 0926. What do you think?
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant miry of patients who have acute coronary occlusion.”
Triage EKG: What do you think? Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Pain largely resolved prior to EMS arrival but completely subsided after prehospital NTG and aspirin. A prior ECG was available for comparison. There is STE present in leads V2-V5. ng/mL (undetectable).
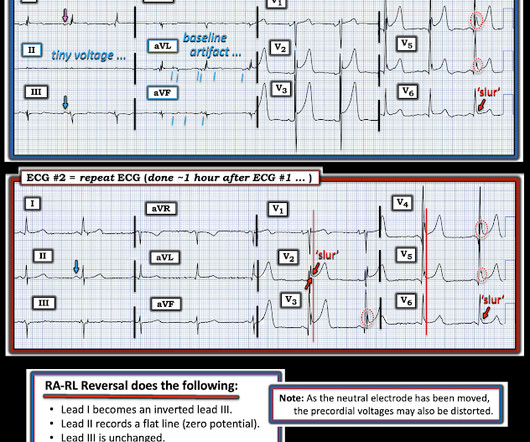
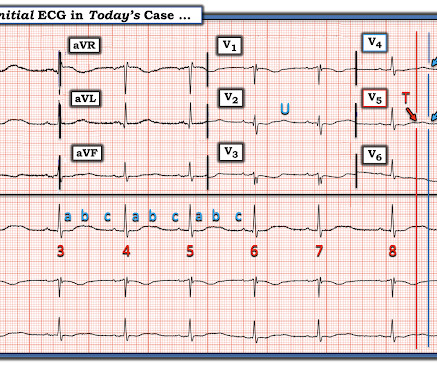
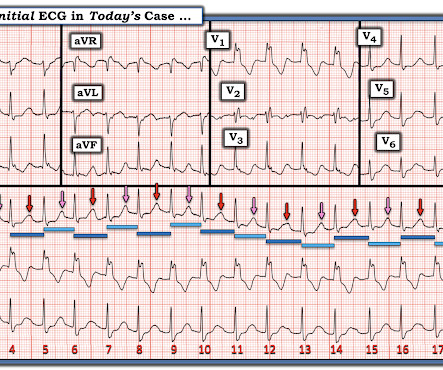
Written by Magnus Nossen and Ken Grauer ( with Comment by Smith ) The ECG in Figure-1 was electronically transmitted by the ambulance service for evaluation. He was hemodynamically stable at the time ECG #1 was recorded. QUESTIONS: How would you interpret this ECG? Figure-1: The initial ECG in today's case. ( in duration.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
This month, after a few months of primarily medical topics, we’re talking trauma, specifically Blunt Cardiac Injury: EmergencyDepartment Diagnosis and Management. Jeff: And don’t forget to get the crash details from the EMS crew before they depart! New EKG findings requires admission for monitoring.
Duchenne Muscular Dystrophy (DMD) is a complex and progressive disease requiring highly specialized care, especially in emergency situations. When patients with DMD present in the EmergencyDepartment (ED), an understanding of the nuanced aspects of their care is essential for optimal management. Orphanet J Rare Dis. Pediatrics.
1: How to Spot Ischemia in RBBB Patients Spoon Feed In non-ischemic right bundle branch block (RBBB) ECGs, we expect discordant ST depression and T wave inversions in leads V1-V3. Follow Dr. Clay Smith at @spoonfedEM , and sign up for email updates here. #1: Try this checklist!
Computer interpretation of the ECG has been called a double-edged sword: when correct, it increases physician accuracy, but when incorrect it increases errors. This is especially problematic in the emergencydepartment, where computer accuracy drops as clinical significance increases—with common errors for arrhythmias and ischemia.
Authors: Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA), Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
3 Always get an EKG to assess for cardiotoxicity, including widened QRS and prolonged QTc, although this may not be evident right away. 3 Cardiotoxicity 3 All patients need an EKG and cardiac monitoring. Case Follow-up: The patient required a dose of lorazepam in the emergencydepartment. EMIT II immunoassay).
Patients with OMI have higher mortality and worse left ventricular function than those with NOMI, making detection crucial but challenging in busy emergencydepartments. OMI signs on ECG include subtle ST elevation, isolated ST depressions, and hyperacute T waves, often missed under current STEMI criteria.
Show Notes Please click here and take our listener survey EmergencyDepartment management of Non-St Segment Elevation Myocardial Infarction, by Drs Julianna Jung and Sharon Bord. Part 4: Pre-hospital care Prehospital ECGs decrease time to intervention. Diagnostics Telemetry ECG. Patterns to know… Troponin.
He is […] The post SGEM#337: Amazing GRACE-1 How Sweet the Guidelines – Recurrent, Low Risk Chest Pain in the EmergencyDepartment first appeared on The Skeptics Guide to Emergency Medicine. Date: July 1st, 2021 Guest Skeptic #1: Dr. Chris Carpenter is Professor of Emergency Medicine at Washington University in St.
A gravid woman presents to your emergencydepartment (ED). 1 If HR is below 60, chest compressions should be started and an ECG placed. Turner , originally trained at the Medical University of South Carolina, is an EM intern at Hershey Medical Center in Hershey, Pa. Garvey AA, Dempsey EM. Adv Med Educ Pract.
Risk Factors Prehospital Care – what should EMS be looking for? Table 3 ADD-RS score Exam Diagnostics Labs EKG – STEMI? Risk Factors* Prehospital Care – what should EMS be looking for? * It is in Beta and your feedback is welcome. It is in Beta and your feedback is welcome. Table 3ADD-RS scoreExamDiagnosticsLabsEKG – STEMI?
But this month’s episode is special in its own way - we’ll be tackling Electrical Injuries in the emergencydepartment - from low and high voltage injuries to the more extreme and rare lightning related injuries. Jeff: Let’s move on to evaluation in the emergencydepartment. Jeff: You’re right. Let’s move on to treatment.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content