This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
On a busy day shift in the emergencydepartment, our seasoned triage nurse comes to me after I finish caring for a hallway patient, “Hey, can you come see this guy in the triage room? Our nurse did not study Paul Ekman’s Facial Action Coding System for Action Units to code “fear” in the patient’s face.
James Broselow, a family medicine-turned-emergency medicine physician from Hickory, North Carolina , recognized that his team spent a lot of time trying to calculate doses of medications rather than spending their mental energy on the actual medical decisions for the resuscitation. Academic Emergency Medicine, 14: 500-501.
You’re in the paediatric emergencydepartment, typing some notes for the child you’ve just discharged. Then you hear the words coming out of the speaker, “ Paediatric code black. Paediatric code black ”. You’ve heard the phrase code black before – it’s a traumatic cardiac arrest. Resuscitation is a team sport.
This time we have our first group of colleagues from Birmingham Children’s Hospital EmergencyDepartment. Intranasal fentanyl and discharge from the emergencydepartment among children with sickle cell disease and vaso-occlusive pain: A multicenter pediatric emergency medicine perspective. Am J Hematol.
MTP logistics include details such as who will be delivering the blood, what actually goes in each cooler, what ratios should be used, limitations imposed by the use of frozen plasma, and documentation. Documentation is critically important, both in the trauma bay and the blood bank. And there are plenty around all the time!
In most EmergencyDepartments, staff are allotted little of that scarce resource, time, to begin processing what has just occurred. These unprocessed emotions can lead to vicarious trauma , especially in resuscitation providers. The Pause Jonathon Bartels worked as an Emergency Nurse in America in 2009. Resuscitation.
Before nitroglycerin (NTG) could be administered, the patient became unresponsive and was transferred to the resuscitation bay, where the monitor revealed a ventricular fibrillation arrest. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. N Engl J Med. 1992;326(22):1451-1455. Circulation.
Over the past few years, there has been an increase in emergencydepartment (ED) volumes and lengths of stay. The effect of emergencydepartment crowding on lung-protective ventilation utilization for critically ill patients. Unfortunately, its not clear whether the documentation came from RTs or ED providers.
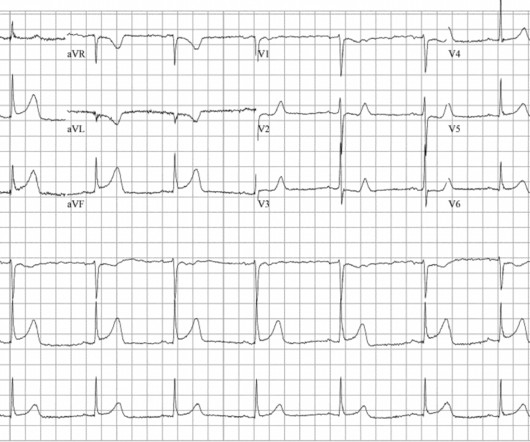
Airway plan discussed with resuscitation team. Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. Cric is progression of the airway plan ; it is not a failure.
He is an assistant professor in Emergency Medicine, Neurology, and Neurosurgery at the School of Medicine at the University of Washington. Case: A 65-year-old man is brought into the emergencydepartment (ED) by emergency medical services (EMS) after his family saw him slump over at the dinner table.
While a randomized control trial should be done to evaluate the effect of early proning in a controlled environment, these studies suggest that we should consider using this in our EmergencyDepartment for patients who present with hypoxia and concern for mild to moderate ARDS without urgent need for intubation. Crit Care Med.
pdf Equipment required for resuscitative thoracotomy: Surface anatomy: Appearance of pericardial clot A foley catheter being used to fill a cardiac wound – note how easily this could be pulled out. An open chest with aortic compression Simulation of resuscitative thoracotomy by London HEMS team. Resuscitation; 2011: 1194-1197
Maimonides Medical Center (MMC) is Brooklyn’s largest hospital, an academic quaternary care center with, in normal times, 711 total beds, 66 intensive care beds, and an EmergencyDepartment that treats approximately 120,000 patients per year. and Emergency Medicine residents, in 12 hour shifts.
But less physicians talk about the difficult “firsts” like failing your first test, losing your first patient, or being involved in your first code. It means a patient is dying and requires immediate resuscitation. I remember my first code blue like it was yesterday. Thirty minutes after he arrived a code blue was called.
If pre-made syringes are not financially feasible then the creation of these medications should be done by a dedicated emergencydepartment pharmacist. Clinical Bottom Line: Acute hypotension must be treated emergently in order to decrease morbidity and mortality. J Med Toxicol. Epub 2019 Jul 3. Intensive Care Med.
Written by: Diana Halloran (NUEM ‘24) & Andrew Long (NUEM ‘25) Edited by: Nick Wleklinski (NUEM ‘22) Expert Commentary by : John Bailitz, MD Introduction The EmergencyDepartment is a challenging work environment for a variety of reasons. Any team member of the resuscitation may lead the hot debrief.
A middle-aged male with squamous cell carcinoma and extensive metastases is brought to the emergencydepartment (ED) after being found unresponsive following a believed suicide attempt (SA) by methadone ingestion. You want to respect patient autonomy, but is it legal to let him die without any emergencyresuscitation?
of patients with follow-up documentation, 70.8% (95% CI 62.9–77.9) Data collected were the worst values documented within the same calendar day as the blood cultures were obtained. The mean time to randomisation was 2 hours, which excludes the initial resuscitation window. Of the 74.9% 1872 children (mean age 2.5
This month, after a few months of primarily medical topics, we’re talking trauma, specifically Blunt Cardiac Injury: EmergencyDepartment Diagnosis and Management. Post opiate hypotension in prehospital trauma patients is a rare but documented complication. Ann Emerg Med. Let’s move on to treatment. 2006;48(3):227-235.
This month, we are sticking in the abdomen for another round of evidence-based medicine, focusing on EmergencyDepartment Management of Patients With Complications of Bariatric Surgery. Vitamin D, B12, Calcium, foate, iron, and thiamine deficiencies are all well documented complications.
By Christy Rukamp DO and Zachary Hampton DO At times, documentation feels like the bane of existence. In residency, we practice resuscitations, rehearse critical procedures, and review in-service test questions; however, we rarely learn key components of documentation. It is more than a record of the patient’s ED timeline.
Epi vs. NorEpi Spoon feed: Continuous epinephrine infusion for post-resuscitation shock in out of hospital cardiac arrest (OHCA) was associated with both higher all-cause and cardiovascular specific mortality when compared to norepinephrine. Check out journalfeed.org for details.
Interestingly, one retrospective study found limited agreement between EMS records and hospital documentation on current DOAC usage. Jeff: For all agents, regardless of the DOAC, the initial resuscitation follows the standard principles of hemorrhage control and trauma resuscitation. Nachi: So I think that rounds out testing.
Neil Dasgupta is an emergency physician and ED intensivist from Long Island, NY, and currently an assistant clinical professor and Director of Emergency Critical Care at Nassau University Medical Center. Case: A code blue is called for a 71-year-old male in-patient that is boarding in the emergencydepartment (ED).
Case: You are working a regular shift in the emergencydepartment when you hear a code blue called. You are the first physician to respond and you begin to resuscitate the patient. Cardiac Arrest: Pulselessness requiring chest compressions and/or defibrillation, with a hospital wide or unit based emergency response.
Guidance documents College of Paramedics Statement on Intubation, available here. Emergency tracheal intubation: complications associated with repeated laryngoscope attempts. Association Between Repeated Intubation Attempts and Adverse Events in EmergencyDepartments: An Analysis of a Multicenter Prospective Observational Study.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. Electrical injuries in the emergencydepartment: an evidence-based review. Emerg Med Pract.
Other things listed on tags can be a patient’s name, bar code, MRN or other tracking criteria. These patients are expected to decompensate within the hour but did not need immediate resuscitation [2]. Hospital-Based Emergency Care: At the Breaking Point. In theory, this is a good way for patients to be tracked and accounted for.
It is critically important to document the physical findings in a plain-seeing, plain-speaking, non-judgmental manner that will not color or taint future investigations. Accurate time entries are important to document. Ballistic injuries in the emergencydepartment. Emergency medicine practice, 13(12), 1-30.
used BNP in the emergencydepartment to differentiate heart failure from respiratory causes in infants and children with heart failure and those with no past medical history. for the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Cohen et al. Later, Maher et al. Am J Cardiol.
CT is good but you really should learn ultrasound, and lastly, sick patients need prompt consultation and resuscitation, not rapid trips to radiology. Unstable patients do not belong in a radiology suite - they belong in the ED resus bay to be resuscitated first. PA’s and NP’s - make sure to use the code APP4 at checkout to save 50%.
A Rising Troponin That afternoon, he complained of increased shortness of breath and was noted to have oxygen saturations in the 70s, prompting a mini code to be called. He became pulseless on more than 1 occasion ( presumably in EMD ) — but responded to resuscitation + treatment with pressors, by regaining a pulse with a spontaneous rhythm.
Written by Destiny Folk MD, with edits by Meyers, peer reviewed by Smith and Grauer A woman in her late 20s with a past medical history of cervical cancer status post chemotherapy and radiation therapy presented to the emergencydepartment for shortness of breath, chest tightness, and two episodes of syncope.
ABG and VBG Correlation The correlation between venous and arterial blood gases is well-documented for standard differences (Table 1), and the data obtained from the VBG can be acted on as if it were an ABG (1, 3-6). In contrast, ABG and pH alone are not reliable in determining the clinical futility of resuscitation after major trauma. (14,
This is the fifth part of our series on "Early Modern Resuscitation." " Part I: Oral Airways, early resuscitation, and recognition of airway care. It was not a practical resuscitative aid until production could be commercially successful (~1895) and made portable in compressed form. Pulmotor is 1907. Beecher, M.
Comparison of the MASCC and CISNE scores for identifying low-risk neutropenic fever patients: analysis of data from three emergencydepartments of cancer centers in three continents. Application of the MASCC and CISNE Risk-Stratification Scores to Identify Low-Risk Febrile Neutropenic Patients in the EmergencyDepartment.
saline (NS) solutions are both isotonic crystalloids widely used for intravenous fluid resuscitation across many contexts and disease states ( Myburgh 2013 ). PMID: 39250114 Clinical Question: In adult patients admitted for a vaso-occlusive episode, does early fluid resuscitation with Lactated Ringer solution compared to 0.9%
The protocol below does not apply to resuscitation patients. For resuscitation patients, see The First Five Minutes of Resuscitation. I see one patient at a time, and I document after each patient. Is this a resuscitation patient improperly assigned to a non-resus priority? Review at the vital signs.
then need further evaluation Usually with CTA imaging If normal physical exam & ABI>0.9, then need further evaluation Usually with CTA imaging If normal physical exam & ABI>0.9, million presentation to ED’s throughout the US Usually occur due to falls Also commonly occur due to sports, MVC’s, etc.
Around the world, acute pain is the most common reason for patients to present to the emergencydepartment (ED). Emergency physicians do not usually perform procedures on hospitalized patients, except for cases where there is a critical need such as intubations, central venous access, and cardiopulmonary resuscitation.
She presented to the EmergencyDepartment at around 3.5 The note documents that the first view of the LCX showed 99%, TIMI 2 flow, but then (before intervention) was seen to fully occlude in real time (100%, TIMI 0). The chest pain was described as severe pressure radiating to both shoulders. hours since onset.
Work-up and Diagnosis in the EmergencyDepartment Initial presentation of TLS typically includes generalized symptoms such as gastrointestinal distress, decreased appetite, muscle cramping, palpitations, hematuria / oliguria, and altered mental status. original document created by author of post. in females and 2.5-7.0
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content