This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
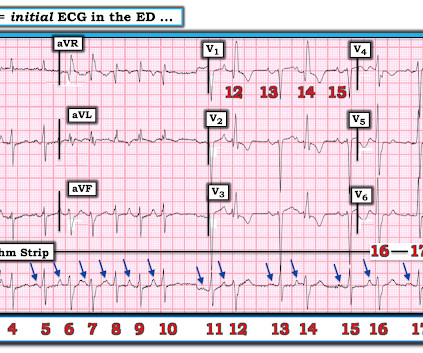
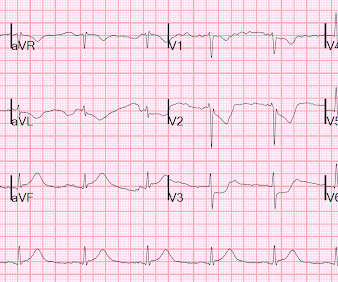
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. If this EKG were handed to you to screen from triage without any clinical information, what would you think? Do you appreciate any dynamic changes compared to the patient’s prior EKG? What do you think? In fact, Kosuge et al.
A young man presented with a gunshot wound to the right chest, with hemo-pneumothorax and hemorrhagic shock. But he did get an EKG: What is this? Figure-1: The ECG sent to Ken Grauer ( showing some semblance of "group" beating ). He got a chest tube and intubation and massive transfusion and stabilized. Formal echo was normal.
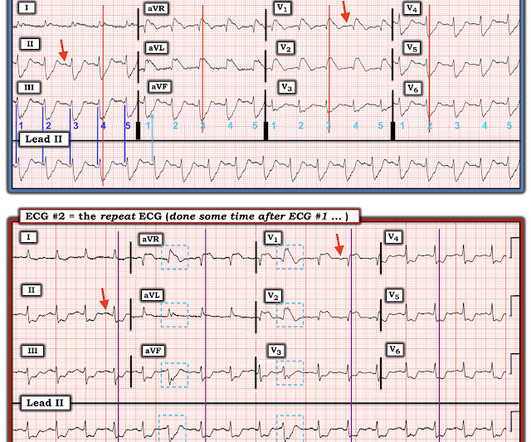
The first EKG is from 2:30 PM on the day of presentation to the ER. My eyes would bulge within a second of viewing this ECG. I texted this to our group "EKG Nerdz," asking "Do you think that anyone could miss this?" No repeat ECG was recorded. The EKG was not repeated until 7 AM the next morning, about 16 hours later.
A 20-something presented after a huge verapamil overdose in cardiogenic shock. mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave).
An ECG is performed and is shown below: Figure 1. Adapted from Dr. Smith’s EKG Blog. Another ECG is obtained and shown below. Source: [link] As you are calling the ICU and cardiology team, the patient has recurrence of her symptoms and repeat ECG shows return of the PVT. She denies chest pain. What do you do?
Initial ED ECG: What do you think? Then we must consider clinical data other than the ECG, for a pretest probability : Of all wide complex tachydysrhythmias, the majority are VT. Shocked x 2 without effect. Warning: if this is VT, a calcium channel blocker can result in shock and death. Why did I say that? What to do now?
Here are his EMS ECGs along with the Queen of Hearts interpretations below each one: EMS1 0650 EMS2 0707 Click here to sign up for Queen of Hearts Access The ECGs show RBBB and LAFB, with small but important concordant STE in V2. In EMS2 ECG, the T waves in V5 is possibly hyperacute. So the cath lab was activated.
Add into this that the majority of children will be in normal sinus rhythm (NSR) by the time of assessment so to truly identify those who have something wrong we have to be confident in identifying arrhythmias where they are present and critical when analysing an ECG in NSR. All were examined and 98% had an ECG.
A closer look, though, also shows the technology of the daya bulky, two-way radio for communicating with EMS, metal gurneys, glass saline bottles, and portable ECG monitors the size of a small shopping cart. Notice the use of the medical anti-shock trousers and the ECG machine. Click to enlarge.) I like the excitement.
The below ECG was recorded. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. This ECG does not have the typical ST-vector of an LAD occlusion. See below for Ken Grauer Comment on the initial ECG: == On arrival, another ECG was recorded: There appears to have been quite a bit of spontaneous reperfusion!
He had the following EKG recorded: Low voltage, suggests effusion. A Rising Troponin That afternoon, he complained of increased shortness of breath and was noted to have oxygen saturations in the 70s, prompting a mini code to be called. Assessment was severe sudden cardiogenic shock. He remained hypotensive and in shock.
The baseline ECG is basically normal with no ischemia. Here is what the Queen of Hearts says about the Baseline ECG: Active chest pain triage ECG also read as not OMI: She says "not OMI", but she does not have access to the baseline ECG. In the future, we will be able to have her compare with previous and serial ECGs.
These diagnoses were not found in his medical records nor even a baseline ECG. He had no previously documented medical problems except polysubstance use. An ECG was obtained shortly after arrival: What do you think? There is no evidence of WPW on this ECG, but it is diagnostic for OMI. What are we seeing here?
She was in shock with thready pulses. A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy? The rate is not fast enough to be causing shock, so if it is VT, the priority is still to treat hyperK and secondarily to cardiovert. They thought it was VT, but did not shock. The K returned at 7.4
The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. How do you interpret the below ECG?
An immediate 12-lead EKG was obtained: There is ST elevation in leads aVR and V1, with marked ST depression in I, II, III, aVF, V3-V6. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What should be done? Should the cath lab be activated?
If you or your patient do not have a watch capable of providing you with an ECG, consider asking those on board to allow you to borrow theirs. Get a blood gas when possible to help guide your ventilation. Some newer AED's have the capability of providing you with a rhythm strip.
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Sodium Chloride or Hartmanns if indicated, monitoring for signs of shock. Provide detailed documentation of the initial assessment, treatment provided, and the patient’s response to interventions.
Triage ECG: What do you think? Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Queen of Hearts interpretation: The cardiologist initially was not convinced, stating the ECG was not diagnostic or could not be diagnostic because it was paced.
morbidity and mortality - faculty case follow-up - R4 Capstone - high-risk, low prevalence diseases in pediatrics morbidity and mortality WITH dr. moulds Syncope Complete heart block is a rare but important cause of syncope P waves outnumbering QRS complexes should clue to you to high grade heart block Triage EKGs are often obtained to screen for cardiac (..)
A 12 lead ECG was obtained by EMS and is shown below: What do you think? The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern).
The paramedics found the patient with ROSC and a GCS 7, and an ECG showing LBBB with possible lateral ST elevation. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Below is the first ED ECG, labeled LBBB by the machine. Vitals were HR 58 BP 167/70 R20 sat 96%.
He had an ECG in clinic which worried the providers because of possible inferior MI, and they sent him to the ED. Here is that ECG: What do you think? He was sent to the ED and had this ECG at t = 1 hour: Similar There are several issues which mitigate against acute inferior MI, and these are the Learning Points: 1.
Individualize the choice of using inotropes, vasopressors, or fluids to treat post-CA hypotension and to target the likely cause(s) contributing to the shock and hemodynamic state (100%, 23/23). In patients with enteral intolerance or shock, start with trophic EN (rates of 10–20 mL/h) and adjust according to tolerance (91%, 19/21).
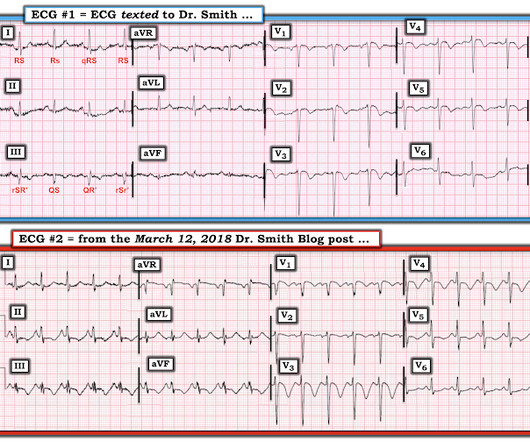
An ECG was texted to me (Smith) without any clinical information: What did I say? Some providers were worried about ACS because of this ECG. It turns out there was a previous ECG for comparison, which I did not see for weeks afterwards: Sinus rhythm with PACs, one is aberrantly conducted. This is NOT Wellens. The answer was yes.
You are tidying your things in anticipation of the arrival of the dayshift when a code blue is called. The patient is in ventricular fibrillation, and you achieve return of spontaneous circulation (ROSC) on the second shock. A post-arrest ECG doesn’t show any signs of STEMI. The patient is still unconscious.
Consider valvular injury in any patient who appears to be in cardiogenic shock, has hypotension without obvious hemorrhage, or has pulmonary edema. Post opiate hypotension in prehospital trauma patients is a rare but documented complication. New EKG findings requires admission for monitoring. of those patients.
Electrical injuries—excluding lightning injuries—account for roughly 10,000 nonfatal shock incidents a year and 500 deaths a year. 1,4-5 Thus, an electrocardiogram (ECG) and cardiac monitoring should be performed for unstable, electrical injury patients. 7 Thus, an ECG is recommended for all electrical injuries. Emerg Med Pract.
Here is the ECG: What do you think? See below how this has been documented. Shah and Rubin studied the computer rhythm interpretation of 2160 12-lead ECGs, compared to 2 cardiologists [ 18 ]. noted computer over-interpretation (false positives) of AF in 9 to 19% of ECGs [ 19 ]. Among, 2447 ECGs, Mant et al.
Essentially there was no difference, meaning we wouldn’t expect to find a difference in outcomes Although not patient oriented, why is there no breakdown of how many patients had cardiogenic shock, congestive heart failure, echocardiographic findings, or even troponin levels. Low O2 protocol: 3.1% aOR 0.96, 95% CI 0.86 Low O2 protocol: 10.6%
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. A near 60 year old male called 911 for increasingly severe fever and SOB.
Given her reported chest pain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Given her tachycardia and episodes of syncope, the patient was judged to be in compensated obstructive shock with very high risk of imminent decompensation. For clarity in Figure-1 — I've reproduced her initial ECG.
He appeared to be in shock. Here is his ED ECG: There is obvious infero-posterior STEMI. This subsequent ECG was recorded after the K was up to 2.2 The QT is much shorter There are now clear U-waves in V2 and V3 2 days later, this ECG was recorded with a K of 3.5: He was managed medically with Clopidogrel.
Electrocardiography (ECG) should be performed on any patient with significant blunt chest injury. A negative ECG is highly consistent with no significant blunt myocardial injury. Any patient with a new abnormality on ECG (dysrhythmia, heart block, or signs of ischemia) should be admitted for continuous ECG monitoring.
Nachi: Moving on to blood pressure: frank hypotension should make you immediately think of a ruptured AAA or septic shock 2/2 an intra abd infection. You can also use the shock index, which as a reminder is simply the HR/SBP. The greatest value of a lactate level is to detect occult shock and sepsis. In one study, a SI > 0.7
Vitamin D, B12, Calcium, foate, iron, and thiamine deficiencies are all well documented complications. Consider performing a RUSH exam (that is rapid ultrasound for shock and hypotension) to identify the cause. Nachi: Check an EKG immediately after arrival for any patient that may be concerning for ACS.
Jeff: There are a shocking 22 million past-month users of marijuana in the US, followed by pain relievers at 3.8 In fact, cannabis use has been documented for medical use dating as far back as 600 BC in West and Central Asia. Jeff: For any patient arriving with suspected cannabis or synthetic abuse, consider checking an EKG.
As part of the workup, she underwent an ECG. Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. We repeated the ECG: Brugada pattern is mostly resolved. Is this Type 2 Brugada syndrome/ECG pattern?
High enough that a bland ECG is not immediately reassuring. ECG 1 What do you think? To me, this ECG is not diagnostic. But if you call every ECG that looks like this OMI, you are going to have a lot of false positives. No further ECGs were obtained for the rest of the day. in absolute terms!
Here is her triage ECG: What do you think? The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR). Here is her ECG 8 hours later: Almost back to normal.
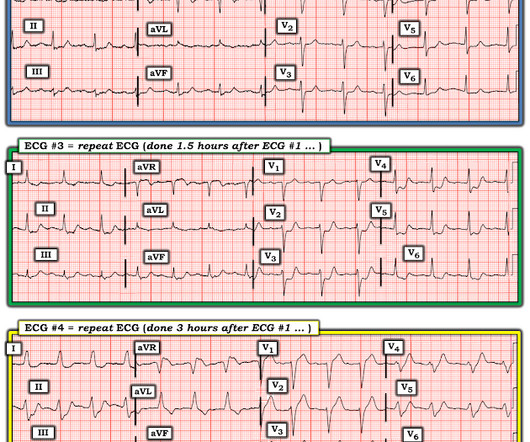
His ECG obtained around 8 AM is shown: ECG 1 My guess is most blog readers will make this diagnosis without too much difficulty. There was no repeat ECG. There is very scarce documentation, but the next ECG was obtained around 1 PM. ECG 2 Diagnostic for inferoposterior reperfusion. ECG 3 Re-occlusion.
Her first ECG is shown. After this ECG was obtained, the ER physician received word that the patient's husband had died in the crash. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Overall bland.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content