
Torsade in a patient with left bundle branch block: is there a long QT? (And: Left Bundle Pacing).
Dr. Smith's ECG Blog
JANUARY 2, 2025
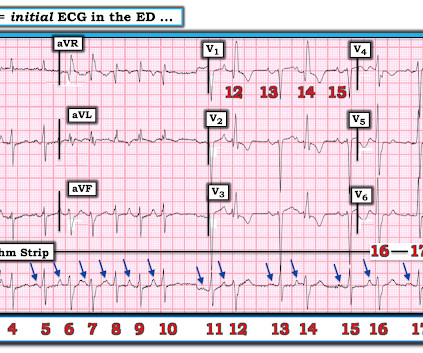
She was managed for sepsis with antibiotics including azithromycin, had hypotension with arterial and central lines placed and pressors. She had an ECG recorded: This is left bundle branch block (LBBB), with appropriate proportional discordance. Bedside cardiac ultrasound showed moderately decreased LV function.



















Let's personalize your content