This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
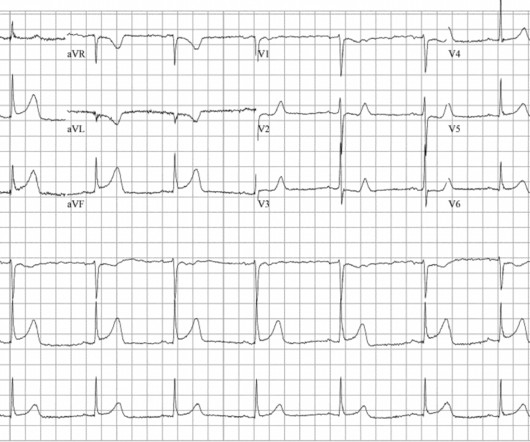
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
Written by Jesse McLaren A 50 year old presented to triage with one hour of chest pain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. see reference below) Whats the gold standard for ECG interpretation: is it cardiologist interpretation? What do you think? The latest is Langlois-Carbonneau et al.
Unless you’re documenting something hilarious, please keep it brief and to the point. History of Presenting Complaint In this section use SOCRATES to document the pain. Drugs/Allergies When documenting drugs – try to get the dose and frequency (this can be found on Summary Care Records from the GP if you have access).
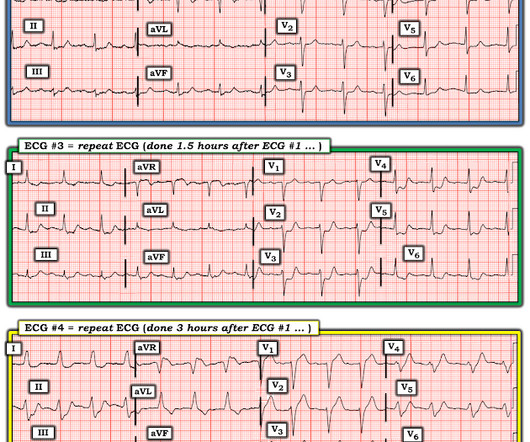
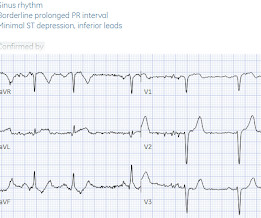
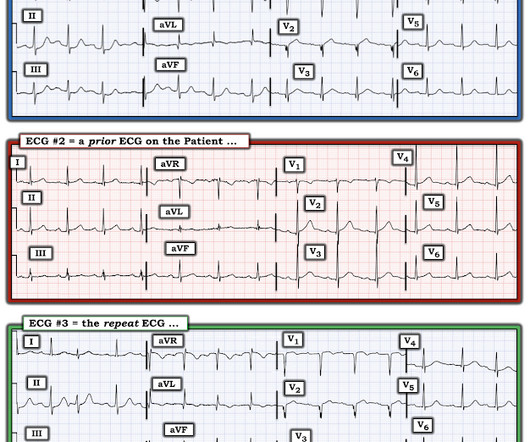
Below are serial ECGs focusing on the inferior leads and aVL. First, what’s the interpretation of each ECG on its own? #1 2 Normal ECG #3. 2 Normal ECG #3. But 90 minutes later troponin returned at 70ng/L (normal <26 in males and <16 in females), and a repeat ECG was done (ECG#2) for recurring chest pain.
All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes.
Written by Jesse McLaren Three patients presented with acute chest pain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. It is well known that NOMI usually has a normal ECG or nonspecific ECG.
Don't miss his analysis and assessment of the Queen of Hearts AI OMI ECG bot -- that assessment is at the very bottom of the post. Her first set of vitals were documented: BP 116/57 Pulse 94bpm Respiratory rate 24/min O2 sat 90% on room air Temp 97F She had been cleaning a Jeep in the sun, and was sunburned. But which artery?
Willy is a cardiology fellow with a keen interest in the ECG in OMI. Triage documented a complaint of left shoulder pain. If an immediate EKG was obtained, it was not saved in the medical record. A patient with OMI can have a totally normal ECG!" Cardiology was consulted, and repeat EKG was obtained at around 2:30 AM.
Below is the triage ECG, with a computer interpretation (Marquette 12 SL) of “normal” which was confirmed by the over-reading cardiologist. Should this patient continue to stay in the waiting room, without interruption of the physician to interpret the ECG, because the computer interpretation is normal? What do you think?
Our nurse did not study Paul Ekman’s Facial Action Coding System for Action Units to code “fear” in the patient’s face. Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome?
. #1: Emergent Cath Lab Activations with “Normal” Computer ECG Interpretations Spoon Feed A significant minority of code STEMI patients have an initial normal computer ECG interpretation. Consequently, emergency physicians must remain vigilant to identify signs of OMI regardless of the initial computer ECG interpretation.
Here are his EMS ECGs along with the Queen of Hearts interpretations below each one: EMS1 0650 EMS2 0707 Click here to sign up for Queen of Hearts Access The ECGs show RBBB and LAFB, with small but important concordant STE in V2. In EMS2 ECG, the T waves in V5 is possibly hyperacute. Long term outcome is unavailable.
Add into this that the majority of children will be in normal sinus rhythm (NSR) by the time of assessment so to truly identify those who have something wrong we have to be confident in identifying arrhythmias where they are present and critical when analysing an ECG in NSR. All were examined and 98% had an ECG.
Here was his triage ECG: What do you think? I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2.
This story, while unlikely to reflect the standards of most readers, has a somewhat surprising outcome. EKG, labs, and a CXR are interpreted by the EP as normal. An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. Too much weight was given to the EKG, CXR, and labs.
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Repeat blood work and ECG 0845: repeat trop over 7000.
Here is the initial ECG at 13:17 with no prior ECG in the patient’s chart for comparison: What do you think? This is another version of the same ECG, lower quality, and with an additional filter applied. See Ken Grauer's additional comments about this ECG at the end of the post! The culprit mid LAD lesion was stented.
This was the ECG obtained at triage. This ECG was recorded and was reviewed remotely by a cardiologist: What do you think? The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Next trop in AM.
These diagnoses were not found in his medical records nor even a baseline ECG. He had no previously documented medical problems except polysubstance use. An ECG was obtained shortly after arrival: What do you think? There is no evidence of WPW on this ECG, but it is diagnostic for OMI. What are we seeing here?
The following ECG was obtained. Note that the machine read is "normal sinus rhythm, normal ECG." ECG 1 What do you think? I sent this ECG to Dr. Smith and Dr. Meyers with no clinical context. Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. <0.049 ng/mL).
During initial assessment, an ECG was obtained and revealed ST-segment elevation (STE) in the inferior leads with ST depression anteriorly. Initial ECG demonstrating inferolateral ST segment elevation and anteroseptal depression, just prior to cardiac arrest. The ECG showed ST-segment elevation without obstructive coronary disease.
Triage EKG: What do you think? A prior ECG was available for comparison. Prior EKG from 2 months ago was available: Let's put the precordial leads from the 2 ECGs side by side: Now you can really see the difference. Immediately after the second ECG was performed, the patient's pain resolved completely.
Exam is normal except for tenderness as documented in the diagram. EKG shows atrial fibrillation with a rate of 169. She never had a documented abdominal exam. I just failed to document it. The EP documented seeing the patient and agreed with the ARNP’s plan. Temp is 98.7 and pulse 121. It was benign.
Patients confirmed on ECG to have atrial fibrillation or atrial flutter Patients with HR >120 bpm. Pregnant or incarcerated patients Documentation for systolic BP is incomplete Intervention: Administration of IV calcium within 60 min prior to or 30 min after IV diltiazem administration in patients with AF/AFL with RVR.
The baseline ECG is basically normal with no ischemia. Here is what the Queen of Hearts says about the Baseline ECG: Active chest pain triage ECG also read as not OMI: She says "not OMI", but she does not have access to the baseline ECG. In the future, we will be able to have her compare with previous and serial ECGs.
Pendell and I have taught the queen on over 40,000 EKGs so far. Version 2 will be coming out soon, also taught on an additional 20,000 EKGs. For version 3, we have started teaching her on yet more EKGs. These ones are EKG that the Queen's users uploaded, and on the comments and outcomes that they give.
Administrative data sets are often collected for the purpose of billing, or costing, or administrative organization, and thus are extremely vulnerable to up coding or intentional or accidental omissions. ” For example, mortality is a patient outcome—provided it can be reliably ascertained.
Here’s the EMS ECG, digitized with PM cardio. They arrived in the ED 30 minutes later to meet the cardiology team, where an ECG was repeated: Again no STEMI criteria, and there has been improvement in the deWinter and swirl pattern. What do you think? There’s sinus arrhythmia with normal conduction, normal axis and normal voltages.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardial infarction, probably old." I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." Every note says "no ischemic changes on ECG." Deemed "NSTEMI."
An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD I sent it to my friend, Ken Grauer , who is very meticulous in his ECG reading. I labeled ECG. As we see in ECG #3 — the regular rhythm is NOT sinus, because the P wave is negative in lead II.
Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. Full case details and outcomes are below. His triage at 0127 is the ECG above. Repeat ECG at 0221: Basically unchanged. Physician: "No STEMI."
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. See 2 dozen examples here: Understanding this pathognomonic ECG would have greatly benefitted the patient. Outcome: Patient ruled out for MI by troponins. Is this Wellens' pattern A?
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Provide detailed documentation of the initial assessment, treatment provided, and the patient’s response to interventions. Proper stabilization and detailed communication with the burns centre are essential for optimal patient outcomes.
Triage ECG: What do you think? Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Queen of Hearts interpretation: The cardiologist initially was not convinced, stating the ECG was not diagnostic or could not be diagnostic because it was paced.
At 3:55 AM during that kind of a night shift, this ECG (among many others) was brought from triage for review by my team. We knew only that the ECG belonged to a man in his 50s with chest pain and normal vitals. Here is the computer interpretation: So we have a triage-computer-normal ECG. No prior available.
Below is the old ECG, showing that all these changes are new – including the Q waves. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
The initial tracing (EKG 1) was obtained. Clinician and EKG machine read of acute pericarditis. Paper published: Terminal QRS distortion not found in any ECG of Early Repolarization TQRSD is defined as the absence of BOTH an S-wave and a J-wave in leads V2 or V3. She was reportedly "pacing in her room while holding her chest".
Unless you’re documenting something hilarious, please keep it brief and to the point. History of Presenting Complaint In this section use SOCRATES to document the pain. Drugs/Allergies When documenting drugs – try to get the dose and frequency (this can be found on Summary Care Records from the GP if you have access).
The EMS crew arrives and performs a 3 lead EKG that does not show an ST elevated myocardial infarction. The crew then asks if you want them to transport your father Code 3 with full lights and sirens. Yes * Was the outcome accurately measured to minimize bias? Yes * Was the cohort recruited in an acceptable way?
He had the following EKG recorded: Low voltage, suggests effusion. A Rising Troponin That afternoon, he complained of increased shortness of breath and was noted to have oxygen saturations in the 70s, prompting a mini code to be called. This is the ECG on V-V ECMO: Very little STE He had a lot of troponins measured.
Here is the first ED ECG, with no pain: Sinus rhythm. The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Computerized QTc = 419. It was stented.
You are tidying your things in anticipation of the arrival of the dayshift when a code blue is called. A post-arrest ECG doesn’t show any signs of STEMI. The primary outcome was a good neurologic outcome within six months and occurred in 55% of the hypothermia group and 39% of the normothermia group (p=0.009, RR 1.40, 95% CI 1.08-1.81).
Here is his initial ECG: 00:04 What do you think? With no other information other than the first ECG above, I texted this to Dr. Smith and he responded: ST elevation in lead V2 and terminal QRS distortion in V3. Therefore, this ECG would not have met the criteria for ACO by this formula. LAD occlusion. Great case.
CESAR Trial Published in 2009 Found that even those who didn’t get ECMO, but were transported to a tertiary care center had better outcomes No matter where you go, critical care transport will be part of your life as a sending physician, receiving physician, or both. Benefits of transport are evidenced based.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content