This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
” Yes, I have seen clerking look like this and I can confirm, it does not go down well. Unless you’re documenting something hilarious, please keep it brief and to the point. History of Presenting Complaint In this section use SOCRATES to document the pain.
The facility does not have ultrasound (US) availability at the time of the patient’s presentation, as the sonographer comes to the hospital only 2 days a week. First, examine the patient and risk-stratify them for the diagnosis of DVT before deciding on the clinical utility of an ultrasound. What findings make a DVT more likely?
You can read the document here. Read the original document here. Ultrasound Is Upvoted The panel weakly suggested bedside ultrasound for patients with fever and an abnormal chest radiograph, but only if an expert is available to interpret the often complex or borderline results. What’s a Fever?
Ocular point-of-care-ultrasound (POCUS) was performed as seen below. Our patient underwent anterior orbitotomy, but there are case reports in the literature of ultrasound-guided drainage (4). In addition, there are studies that discuss missed cases of abscess on CT that were detected with use of ultrasound. Brzycki et al.
The ultrasound-guided clavipectoral plane block (CPB) is a newly described technique in the emergency medicine literature. Ultrasound Survey Scan FIGURE 1A: Ultrasound probe should be placed at the clavicle with the probe marker facing cephalad (toward the head). FIGURE 1B: Ultrasound image with labeled relevant anatomy.
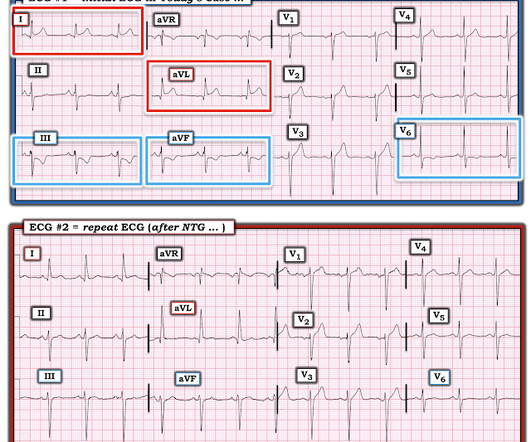
Bedside cardiac ultrasound with no obvious wall motion abnormalities. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." The proximal LAD has mild disease, but the distal LAD and diagonal branches are not well evaluated in this view. The distal LCx is seen, and the OM is not well visualized here.
(1) However, it wasn’t until the 1890s that purposeful, successful, and safe attempts to access this fluid were documented (2). The LP is now a standard procedure and in 2010 well over 135,000 LPs were performed in Emergency Departments throughout the US (3). (And WHY - Why Not?
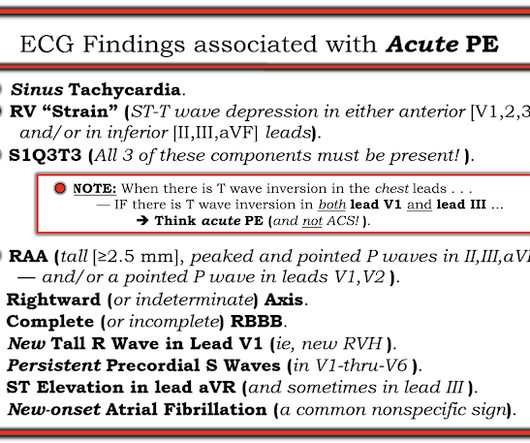
There are well preserved R-waves in Wellens waves. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism. Now another, with ultrasound. Submitted by a Med Student, with Great Commentary on Bias! Chest pain, SOB, Precordial T-wave inversions, and positive troponin. This is a quiz.
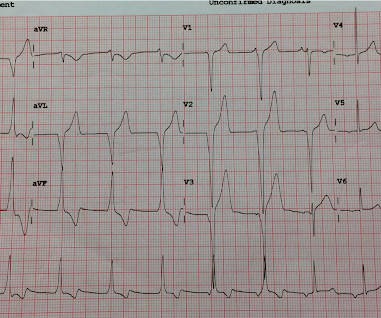
There are findings concerning for anterolateral OMI including ST elevation and hyperacute T waves in the anterolateral leads most prominent in V2-V5, as well as hyperacute T waves in the inferior leads. On our ultrasound machine, the TEX, normal strain is considered -18 % and higher (more negative).
But there had been two placebo-controlled drug trials that documented a 45-55 second increase in exercise time. A later re-analysis increased the time to 21 seconds, which was still well below statistical significance. You might wonder how they came up with 200 patients? This, too, was brilliant thinking.
” Yes, I have seen clerking look like this and I can confirm, it does not go down well. Unless you’re documenting something hilarious, please keep it brief and to the point. History of Presenting Complaint In this section use SOCRATES to document the pain.
He had no previously documented medical problems except polysubstance use. However the patient continued to have chest pain and bedside ultrasound showed hypokinesis of the septum with significantly reduced LVEF. The LCx and OM vessels are not as well visualized. An ECG was obtained shortly after arrival: What do you think?
We discussed some practices to push learners outside of their comfort zone and promote learning, based on their level as well as their goals for the shift.
In both tracings — an exceedingly fast PMVT is documented. In this study — Procainamide was superior to Amiodarone for terminating monomorphic VT, as well as having fewer adverse effects than Amiodarone ( Ortiz et al — Eur Heart J 1;38 (17): 1329-1335, 2017 ). The arrhythmia starts with a PVC having a short coupling interval.
What is your initial imaging test of choice, ultrasound (US) or non-contrast CT, and why? Would you be confident in a point-of-care-ultrasound evaluation or a formal ultrasound? Many patients in the ultrasound groups did get additional imaging, but this was not the majority. How do you proceed? In this study, 40.7%
There is a substantial ANZICS document on tracheostomy that forms the structure for this tasty morsel. And this seems to work exceptionally well. I suppose this is somewhat similar to ultrasound for CVCs as plenty of people seem to cope perfectly well without it * no good data to guide a solid recommendation as yet.
The cut points for what constitute OMI and not OMI as well as confidence levels are calibrated to maximize sensitivity and specificity according to the receiver operating characteristic. The diagonal branches are overlapping one another and not well visualized in this view. The QOH output is a number between 0 and 1.
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia.
Pads were placed with ultrasound guidance, so they were in the correct position. As I discussed and documented in Lesson 1 of My Comment at the bottom of the page in the April 2, 2022 post of Dr. Smith's ECG Blog — certain patients may remain in sustained VT not only for hours — but even for days! However, this is not SVT.
A bedside cardiac ultrasound was normal. It appears to be benign in children as well (see references below). He has a great blog too: ECG Interpretation He is also well known on the Facebook EKG Club page , where you can learn tons about ECGs: Here is his response, with the first ECG labelled: Hello Steve & Avinash.
His practice is in trauma, emergency general surgery, and critical care with an academic interest in ultrasound and medical simulation. His practice is in trauma, emergency general surgery, and critical care with an academic interest in ultrasound and medical simulation. first appeared on The Skeptics Guide to Emergency Medicine.
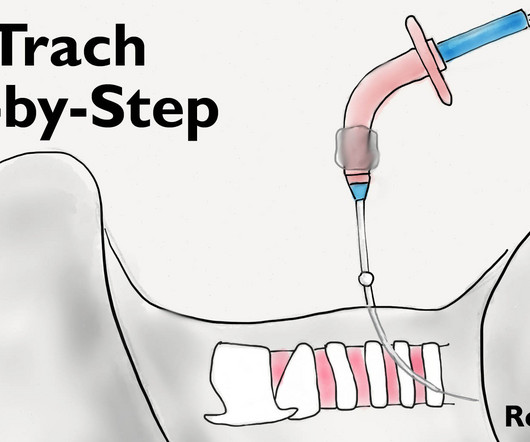
Use ultrasound to identify an large vessels in the area. Dont forget to document your perc trach procedure well. Skin Incision The neck should be carefully palpated and the anatomy should identified (thyroid cartilage, cricoid cartilage, and 2-3 tracheal rings). Consider labelling the landmarks with a permanent marker.
Generally accepted (and some airlines spell it out) that they are assuming the liability even for you helping Documentation: To protect yourself (and the airline), will/should make documentation of what happened. hours earlier and went to OR 3.5 hours earlier and went to OR 3.5 Each airline generally has their own protocol.
This may well seem daunting given how unwell and complex the patients might be but a thorough, well-structured A-E will give you most of the information you need to progress that patient’s care. C Assessment BP and MAP Invasive reading (via an arterial line) or non-invasive (via a BP cuff)?
A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. There was no cough or fever, the CXR looks like pulmonary edema, the ultrasound showed classic pulmonary edema B lines. ECGs were interpreted for OMI, as well as various characteristics of ST depression, blinded to outcomes.
Individualize MAP targets based on the patient, as well as treatments (inotropes, vasopressors, and fluids) for hypotensive patients. These conversations should occur frequently and be clearly documented for other health care professionals who are not present during the conversations (96%, 22/23). There are no hard MAP recommendations.
This child is at risk for expected complications, as well as overdiagnosis and iatrogenia. These children depend on their preload to run blood passively into the pulmonary circuit; afterload reduction is also important to compensate for a poor left ejection fraction, as well as to avoid the development of pulmonary hypertension.
A bedside cardiac ultrasound was performed with a parasternal long axis view demonstrated below: There is a large pericardial effusion with collapse of the right ventricle during systole. This patient was reported to have distant heart sounds but was not hypotensive and did not have JVD according to documentation.
CT is good but you really should learn ultrasound, and lastly, sick patients need prompt consultation and resuscitation, not rapid trips to radiology. Nachi: Diagnosis of appendicitis, in a pregnant patient, ultrasound vs. mri. Jeff: Next we have everybody’s favorite, the ultrasound. Jeff: Indeed. Sounds familiar.
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chest pain radiating to "both axilla" as well as the upper back. The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward.
A natural one, and especially suited for increasing capability without regard to physician residency program output of graduates, and in less-well-served rural areas. Advances in Medical Imaging (CT, MRI, and Ultrasound) facilitating rapid, accurate, diagnosis affording new potential to save additional lives. EDNA->ENA. Sakran, J.
Nachi: This month’s team parsed through roughly 1200 articles as well as guidelines from the eastern association for surgery in trauma also known as EAST. Post opiate hypotension in prehospital trauma patients is a rare but documented complication. Nachi: Definitely. for pericardial effusion.
Trauma patients between the ages of 18-90 years had to have either had one documented episode of hypotension (defined as a systolic BP <90 mmHg) or tachycardia (>100 beats/minute) to be included in the study. If the trauma center performed screening ultrasounds to evaluate for asymptomatic DVTs, they were not included in this study.
Jeff: Well that’s kind worrisome. Which again reiterates why this is such an important topic for us as EM clinicians to be well-versed in. For the sake of completeness, just be aware that there is also the biliopancreatic diversion with or without a duodenal switch, as well as a vertical banded gastroplasty.
Jeff : So as well all know Sepsis is bread and butter emergency medicine, but, what is sepsis? If it’s possible to establish an IV and initiate fluids without delaying transport, EMS should do that as well. One, lung ultrasound can be really useful to find that occult pneumonia or differentiating pneumonia from CHF.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. A late middle-aged man presented with one hour of chest pain.
It was peer-reviewed by Joseph Habboushe, assistant professor at NYU and Nadia Maria Shaukat, director of the emergency and critical care ultrasound at Coney Island Hospital in Brooklyn, New York. In fact, cannabis use has been documented for medical use dating as far back as 600 BC in West and Central Asia.
Nachi: Well, I’m sure more of those studies are still coming. Nachi: Well that was a ton of information and background on the DOACs. Interestingly, one retrospective study found limited agreement between EMS records and hospital documentation on current DOAC usage. But next we should talk about ultrasound. Jeff: Agree.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Vasovagal syncope is generally benign. orthostatic vitals b.
EF does not correlate with particularly well with mortality in sepsis though diastolic dysfunction does * It may be due to under filling and the reduced diastolic filling due to the ubiquitous tachycardia in sepsis. This has relevance to the ICU population in 2 major ares * Sepsis. *
So to get us all on the same page, the discriminatory zone is the b-HCG at which an IUP is expected to be seen on ultrasound. Nachi: Definitely concerning, but this is all the more reason you need to employ our favorite imaging modality… the ultrasound. For a threatened abortion, the os would be closed with an IUP seen on ultrasound.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. A bedside cardiac ultrasound revealed grossly normal to hyperdynamic systolic function with no obvious areas of wall motion abnormalities. Bayes de Luna, A et al.
Literature suggests we should avoid evaluating ocular pressure, though there are no case reports or peer reviewed data documenting extrusion of ocular contents from ocular pressure evaluation in the ED setting. No need for Seidel test if there’s obvious globe rupture.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content