This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Calls to emergencydepartments (EDs) from ambulances to alert them to a critical case being transported to that facility that requires a special response (‘pre-alerts’) have been shown to improve outcomes for patients requiring immediate time-critical treatment (eg, stroke).
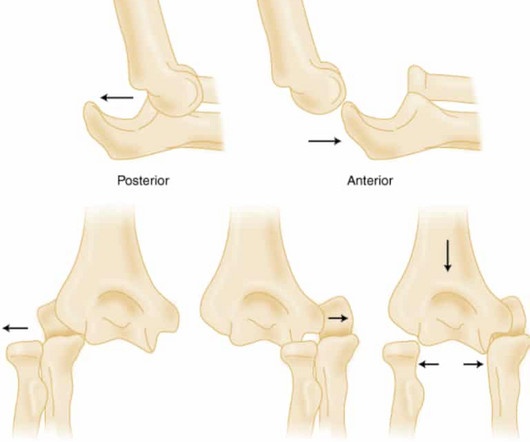
Elbow Dislocations in the EmergencyDepartment: A Review of Reduction Techniques. J Emerg Med. Anatomy, Shoulder and Upper Limb, Radial Nerve. 2023 Nov 5. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 30521261 Gottlieb M, Schiebout J. 2018 Jun;54(6):849-854. doi: 10.1016/j.jemermed.2018.02.011.
About three percent of emergencydepartment (ED) visits are due to skin and soft tissue infections, but data are lacking on the contribution of chronic wounds to this number. Wound management in the ED is only a starting point, and appropriate referral and follow-up are key to an improved outcome. Back to the patient.
Improper care during an emergency This situation can occur in the emergencydepartment when the emergency physician calls a specialist to assist with management. Specialists, make sure you understand the emergency physician’s concerns and clearly explain why you think you don’t need to see the patient in person.
12 How do we address these disparities in the emergencydepartment? 13 Interventions may include: Ascertaining a patient’s preferred language early in the clinical encounter (during registration, for instance), and clearly documenting this preference in a place that is visible to all providers. 45:446-458. Taira B, et al.
.” 1 A study by van Zwieten in 2004 found that 49 percent of deaths attributed to droperidol required dosages 50 mg, magnitudes greater than typical dosages used in the emergencydepartment (ED). outcome of this is the removal of droperidol from the hospital formulary. West J Emerg Med. The realistic (or preferred?)
This story, while unlikely to reflect the standards of most readers, has a somewhat surprising outcome. An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. It wasn’t, so you weren’t called, nor did the doc need to document anything. Baccei SJ et al.
Last month’s article focused on ACEP’s efforts and resources to support EDs and patients with psychiatric emergencies. Emergencydepartments (EDs) focus on rapid initiation of medical treatment. However, rapid initiation of treatment is actually patient-centered care that can both lead to better outcomes and limit ED boarding.
Ventilator-associated lung injury and inflammation can occur even during short-term mismanagement can worsen patient outcomes. Over the past few years, there has been an increase in emergencydepartment (ED) volumes and lengths of stay. This is a critical error that leads to poorer outcomes for patients in need of critical care.
Inhaled Corticosteroids Rarely Prescribed at EmergencyDepartment Discharge Despite Low Rates of Follow-Up Care. J Emerg Med. Among patients with a primary provider documented in the chart, 30-day outpatient follow-up rate was 21.3% (n = 313). The primary outcome was hospital admission rates.
Impact of intravenous calcium with diltiazem for atrial fibrillation/flutter in the emergencydepartment. Am J Emerg Med. What They Did: Researchers conducted a multicenter, retrospective cohort study in three community hospitals and two freestanding emergencydepartments. Article: Rossi N et al. received CaCl 89.3%
The overuse of computed tomographic (CT) scans for patients who present to the emergencydepartment (ED) after mild traumatic brain injury (mTBI) has been well-documented. The Canadian Computed Tomography Head Rule (CCHR) is a validated tool to guide ED providers in determining the need for emergent CT of mTBI patients.
Assessed clinical practice, outcome, length of stay, safety, and efficacy of both phenylephrine and epinephrine peripherally administered through a push dose.
1 Relatively little literature on the clinical characteristics and outcomes of out-of-hospital cardiac arrest (OHCA) patients complicated by coronary vasospasm exists beyond anecdotal reports, however. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented.
Emergencydepartments (ED) represent a promising setting to address preventive health measures like CRC screening. We evaluated feasibility of identification, provided preliminary effect size estimates and documented participant acceptability. The primary outcome was patient CRC screening or scheduling.
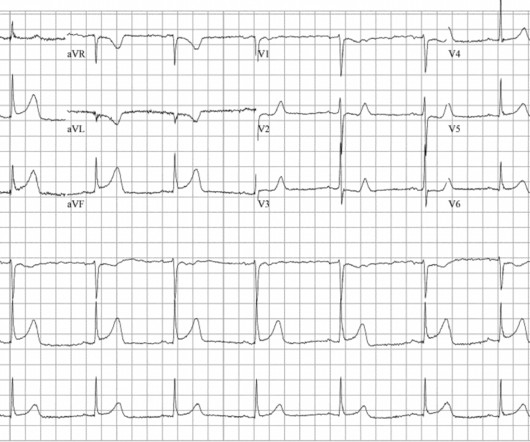
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment.
Maimonides Medical Center (MMC) is Brooklyn’s largest hospital, an academic quaternary care center with, in normal times, 711 total beds, 66 intensive care beds, and an EmergencyDepartment that treats approximately 120,000 patients per year. On March 9, the first patient with a novel coronavirus infection was admitted to MMC.
PECARN prediction rule for cervical spine imaging of children presenting to the emergencydepartment with blunt trauma: a multicentre prospective observational study. A proportion of the patients who were initially missed using the CDR were found to actually have risk factors documented in EMS reports or the medical record.
Reviewed by: Isabella Davenport Article 2: Does it improve outcomes if you replace the nail in nail bed repair? Children with nail bed injuries were randomly assigned to nail replacement or discarding , with the primary outcomes being secondary infection in 7 days and cosmetic outcome in four months. Arch Dis Child.
Outcomes included clinical status when urine culture was available, subsequent antibiotic treatment within seven days and subsequent UTI within 30 days. of patients with follow-up documentation, 70.8% (95% CI 62.9–77.9) The primary outcome was the successful intubation on the second attempt. Of the 74.9% Why does it matter?
Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. The impact of advanced practice provider staffing on emergencydepartment care: productivity, flow, safety, and experience. He is also the CME editor for Academic Emergency Medicine.
Date: March 20th, 2019 Guest Skeptic: Dr.Katie Walker is an emergency physician in Melbourne, Australia. Case: The emergencydepartment is backing up. Your medical team is great, but you […] The post SGEM#250: Scribes – I Want to Break Free (from the EMR) first appeared on The Skeptics Guide to Emergency Medicine.
Emergency thoracotomy in thoracic trauma: a review. EmergencyDepartment thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World Journal of Emergency Surgery; 2006: 1:4. Survival after EmergencyDepartment thoracotomy: review of published data for last 25 years.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. He had no previously documented medical problems except polysubstance use. Annals of Emergency Medicine , 31 (1), 3–11.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. I'll add some thoughts about the first 2 tracings in today's case.
There is a wealth of information relating to best practice in preventing falls and harm from falls, however there is little to guide the accurate prediction of future falls for geriatric patients presenting to the EmergencyDepartment. Predicting Geriatric Falls Following an Episode of EmergencyDepartment Care: A Systematic Review.
Bimodal age of distribution: at birth and 12-18 years 14% of cases occur in adults; older patients have worse outcomes Bell clapper deformity – bilateral in 80% of patients Prior episode of torsion Family history Trauma (can be minor) Clinical Presentation: Sudden/severe testicular pain Often unilateral, may radiate.
This month, after a few months of primarily medical topics, we’re talking trauma, specifically Blunt Cardiac Injury: EmergencyDepartment Diagnosis and Management. Post opiate hypotension in prehospital trauma patients is a rare but documented complication. Early defibrillation is linked to better outcomes. topics.php?paction=showTopic&topic_id=597)
Chief complaints involving the ear are a common occurrence in EmergencyDepartments across the US and include presenting symptoms such as ear pain or fullness, hearing loss, redness, trauma, vertigo, and foreign bodies. A retrospective analysis of the Nationwide EmergencyDepartment Sample (NEDS) from 2009 through 2011 identified 8.6
This month, we’re moving into uncharted territories for the podcast… we’re talking psychiatry Nachi: Specifically, we’ll be discussing Depressed and Suicidal Patients in the emergencydepartment. The strongest predictor for suicide-related outcomes is history of prior suicidal ideation or suicide attempt.
Secondary Outcome By day 90, mortality was 9.3% Strengths: The investigators framed a research question centered on patient outcomes, ensuring the study’s relevance and practicality. Control: Normal Saline via continuous infusion according to the same regimen used in the hydrocortisone group. in the placebo group (p = 0.006).
1 It is a quickly deployable and easily interpreted study that can be done in real time to guide decisions in the EmergencyDepartment. Point of care biliary ultrasound in the emergencydepartment (BUSED) predicts final surgical management decisions. Acad Emerg Med. and specificity of 88.0% 2022;7(1):e000944.
Written by: Diana Halloran (NUEM ‘24) & Andrew Long (NUEM ‘25) Edited by: Nick Wleklinski (NUEM ‘22) Expert Commentary by : John Bailitz, MD Introduction The EmergencyDepartment is a challenging work environment for a variety of reasons.
This month, we are sticking in the abdomen for another round of evidence-based medicine, focusing on EmergencyDepartment Management of Patients With Complications of Bariatric Surgery. Vitamin D, B12, Calcium, foate, iron, and thiamine deficiencies are all well documented complications.
High-dose IN Fentanyl Spoon Feed: Higher doses of intranasal (IN) fentanyl for pain ranging from 2-5 μg/kg (with a maximum of 200 μg) were given in a pediatric emergencydepartment, with no documented episodes of apnea, hypotension, or respiratory failure.
Randomized Double-blind Trial Intramuscular Droperidol, Ziprasidone and Lorazepam for Acute Undifferentiated Agitation in the EmergencyDepartment. Randomized Double-blind Trial Intramuscular Droperidol, Ziprasidone and Lorazepam for Acute Undifferentiated Agitation in the EmergencyDepartment. Reference: Martel et al.
Emergency Physician and Advanced Practice Provider Diagnostic Testing and Admission Decisions in Chest Pain and Abdominal Pain. AEM January 2021 Case: A 50-year-old male presents to the EmergencyDepartment (ED) with left lower quadrant abdominal pain. The patient is seen by an advanced practice provider (APP).
In the end, they reported similar rates of recurrence and bleeding outcomes for acute treatment. Interestingly, one retrospective study found limited agreement between EMS records and hospital documentation on current DOAC usage. This strategy reduces hospital days and costs with otherwise similar outcomes - total win all around.
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergencydepartment, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
A 59-year-old man presents to your community emergencydepartment (ED) with chest pain that is radiating to his back. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Erbel R, Aboyans V, Boileau C, et al.
Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called www.First10EM.com Case: You arrive at 7am to relieve your colleague after a night shift. You find her at the desk, asleep with her face on the keyboard, patient documentation half finished.
Delays in care, as seen in our patient, can lead to poor neurological outcomes (1,2). Chronic compressive or mechanical stress on the spinal cord has been well documented to increase the risk of syrinx and secondary spinal cord changes. Braun P, Kazmi K, Nogués-Meléndez P, Mas-Estellés F, Aparici-Robles F. J Neurosurg. 1995;83(1):1.
Do outcomes for patients with suspected nephrolithiasis differ based on the initial imaging? 1 Low-dose non-contrast abdominal CT has become the gold standard for diagnosis as it has become readily available in emergencydepartments nationwide, with some studies touting sensitivity and specificity of 97% and 95%, respectively.2
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content