This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
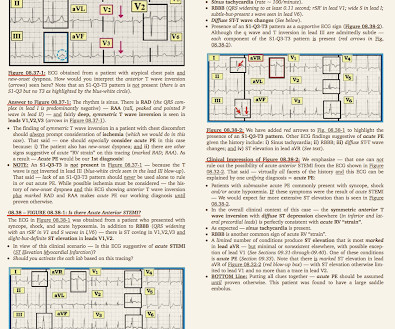
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. Although CP ( C hest P ain ) was not a prominent symptom — ACS ( A cute C oronary S yndrome ) was suspected from the chest lead T wave inversion seen on this ECG. WHY — or Why Not?
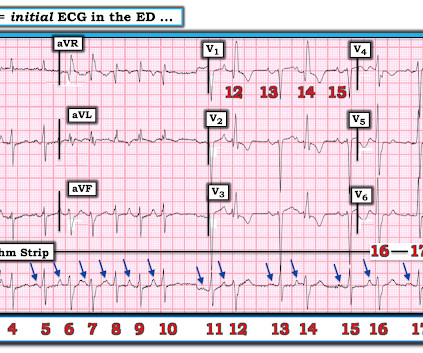
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
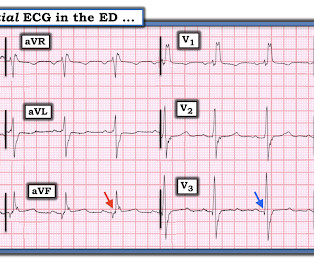
EKG on arrival to the ED is shown below: What do you think? The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. 2) There was no terminal QRS distortion on these ECGs. or basilar ischemia.
The documentation does not describe any additional details of the history. The following ECG was obtained. ECG 1 What do you think? The ECG shows sinus bradycardia but is otherwise normal. There is TWI in lead III, but this can be seen in normal ECGs. The following ECG was obtained around midnight.
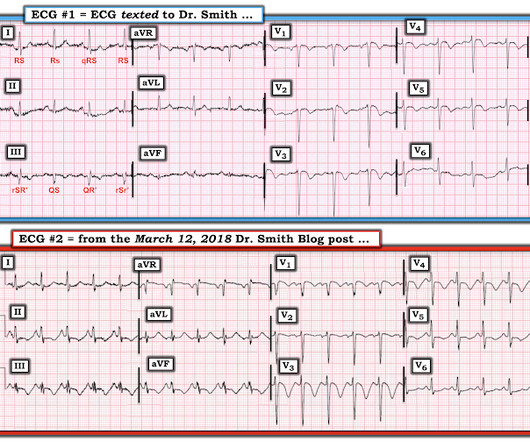
This ECG was texted to me with no other information. The first ECG was recorded at 53 minutes after pain onset. The pain began to improve and this ECG was recorded: T-waves are not quite as tall, though still have a large AUC. An old ECG was found: As you can see, this patient has zero baseline STE, and normal T-waves.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He had a previous ECG on file: Proving the findings are new The cath lab was activated. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. No other symptoms.
She is well appearing, and while being placed on the monitor becomes anxious stating the symptoms are recurring. An ECG is performed and is shown below: Figure 1. Adapted from Dr. Smith’s EKG Blog. Another ECG is obtained and shown below. If the response is appropriate, get another EKG and assess the QT interval.
I have often written about how an ECG interpreted as "normal" by a conventional algorithm may well be manifesting OMI, or even long QT or hyperkalemia. Shifa Karim and Gabe Keller helped with a project to assess all these ECGs with the Queen of Hearts. The ECG told the story. I wanted to show some of the cases here.
All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). A repeat ECG was performed 2 hours after arrival: QTc prolongation ato 722 ms now with alternating T wave pattern (T wave alternans) I texted this to Smith who responded: “T wave alternans and long QT.
During initial assessment, an ECG was obtained and revealed ST-segment elevation (STE) in the inferior leads with ST depression anteriorly. Initial ECG demonstrating inferolateral ST segment elevation and anteroseptal depression, just prior to cardiac arrest. The ECG showed ST-segment elevation without obstructive coronary disease.
Well, that can be a problem. Sometimes things we do are well grounded in evidence. Things like reading ECGs, echocardiograms, as well as learning to do procedures. Well, do you know the actual trials underpinning this evidence? They sit in a Google document. It will be a working document.
The following ECG was obtained. Note that the machine read is "normal sinus rhythm, normal ECG." ECG 1 What do you think? I sent this ECG to Dr. Smith and Dr. Meyers with no clinical context. Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. <0.049 ng/mL).
His ECG is shown: What do you think? The history thus far is highly suggestive of OMI, so we must study the ECG very closely to see if we can confirm this. The Queen of Hearts does not care about rhythm analysis, she simply looks at the ECG and decides whether it represents OMI or not. He pointed out the precordial swirl sign.
In this study, they found that prone positioning resulted in significant improvement in oxygenation, as well as a 50% decrease in mortality at 28 days (Guerin et. Remove ECG leads and patches. Reattach EKG leads to back. Document thorough skin assessment every nursing shift, and inspect weight-bearing ventral surfaces.
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Repeat blood work and ECG 0845: repeat trop over 7000.
Alkali burns result in liquefaction necrosis, allowing for deeper tissue injury as well as vascular injury that can lead to both local and systemic toxicity [1]. Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Establish IV access and begin fluid resuscitation with 250ml boluses of 0.9%
An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD It appears to be benign in children as well (see references below). I sent it to my friend, Ken Grauer , who is very meticulous in his ECG reading. I labeled ECG. His chest was tender.
Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)?
Her presenting ECG is shown below: ECG 1 What do you think? I had previously run this ECG through QOH in the PMcardio app environment and she reported mid confidence, shown below. You can see that version 2 has a higher number than version 1, hence she sees the ECG as more OMI-like than version 1. I sent this to Drs.
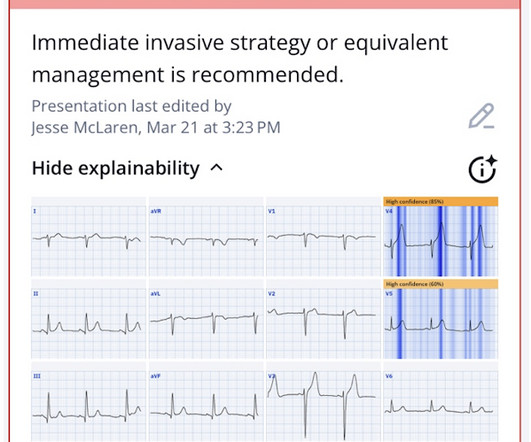
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. See 2 dozen examples here: Understanding this pathognomonic ECG would have greatly benefitted the patient. And ECGs can change and evolve even when there is no ischemia. Is this Wellens' pattern A?
Here is his initial ECG: What do you think? Although diagnostic of MI, it is highly suspicious for " Old inferior MI with persistent ST Elevation" or "inferior aneurysm morphology" because of the well-formed Q-waves and the flat T-waves. The patient's chest pain had resolved by the time of the ECG 2. The T-waves are flat.
Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think? Do you agree with the computer's interpretation of "Normal ECG"? The ECG shows sinus rhythm with normal QRS and R wave progression. This ECG clearly meets STEMI criteria by the way, regardless of age or gender.
It radiated to both shoulders and both upper extremities, and there was shortness of breath and diaphoresis as well. Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardial infarction, probably old." Every note says "no ischemic changes on ECG." Day 2: No ECGs recorded.
At 3:55 AM during that kind of a night shift, this ECG (among many others) was brought from triage for review by my team. We knew only that the ECG belonged to a man in his 50s with chest pain and normal vitals. Here is the computer interpretation: So we have a triage-computer-normal ECG. No prior available.
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chest pain radiating to "both axilla" as well as the upper back. The initial tracing (EKG 1) was obtained. Clinician and EKG machine read of acute pericarditis. What do you think?
This ECG was texted to me in real time, but I did not notice the message until about an hour after it came. "50 This was my response: "This looks like a worrisome EKG. But by now you must have a repeat ECG. But by now you must have a repeat ECG. Another ECG was recorded while waiting for the cath team (it was nighttime).
Here is the first ED ECG, with no pain: Sinus rhythm. The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Computerized QTc = 419. It was stented.
Currently, the infusion of IV calcium before diltiazem is not well understood, and more studies have focused on administering IV calcium prior to verapamil than diltiazem. Patients confirmed on ECG to have atrial fibrillation or atrial flutter Patients with HR >120 bpm. Article: Rossi N et al.
Here is her 12-Lead ECG: There’s a sinus rhythm at around 70 bpm. It is difficult to answer this question based on this single ECG alone. We don’t see excessive ST Elevations (“Tombstones”) that would suggest acute STEMI, but clearly acute STEMI can certainly present with moderate ST Elevation as well.
The triage ECG was sent to me with no history (I did not have access to baseline ECGs), and I said that I thought this was just LVH causing the anterior STE and T waves. I sent this ECG (with no history, no baseline ECG) to Dr. Smith twice, months apart, and he also said LVH without clear OMI. hour delay in this case.
Below is the old ECG, showing that all these changes are new – including the Q waves. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
Here is his initial ECG: 00:04 What do you think? With no other information other than the first ECG above, I texted this to Dr. Smith and he responded: ST elevation in lead V2 and terminal QRS distortion in V3. Therefore, this ECG would not have met the criteria for ACO by this formula. LAD occlusion. Great case.
Here is the result: Next, it interprets the digital data: A perfect interpretation Unfortunately, this ECG was not interpreted as OMI and the patient did not get another ECG recorded until 2 hours later. I tell them that it is not the ECG that is nonspecific, but the interpreter who is nonspecific.
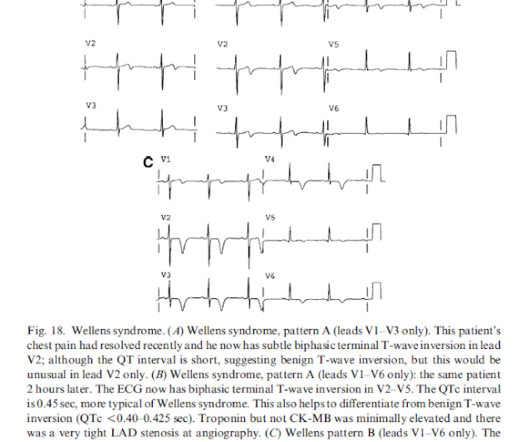
Here was his triage ECG. This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. 90 minutes later, another ECG was recorded: What do you think? BP was 200/100.
This patient presented with vertigo and had an ECG recorded What do you think? But the well-formed Q-wave and the presence of a normal T-wave in inferior leads led me to believe this was Old Inferior MI with persistent ST Elevation, otherwise known as inferior LV aneurysm. Over time, T-waves normalize in the absence of new OMI.
He had a prehospital ECG that was worrisome to the medics, so they called me to see him at the door. His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. and had dilated pupils. He was alert and oriented.
Medical history: History of Ischemic Heart Disease History of Congestive Heart Failure Diabetes Mellitus requiring treatment with insulin Pre-operative serum creatinine >2 mg/dL He had this ECG recorded: What do you think? They compared to a previous ECG and thought they were identical. Are these ECGs of similar risk?
An ECG was texted to me (Smith) without any clinical information: What did I say? Some providers were worried about ACS because of this ECG. It turns out there was a previous ECG for comparison, which I did not see for weeks afterwards: Sinus rhythm with PACs, one is aberrantly conducted. This is NOT Wellens. The answer was yes.
Here is the ECG: What do you think? See below how this has been documented. Shah and Rubin studied the computer rhythm interpretation of 2160 12-lead ECGs, compared to 2 cardiologists [ 18 ]. noted computer over-interpretation (false positives) of AF in 9 to 19% of ECGs [ 19 ]. Among, 2447 ECGs, Mant et al.
Here is his triage ECG: What do you think? We'll simply never know without ECGs from that time period. The extremely high troponin and ECG evidence of LVA morphology are very worrisome long term features for resultant morbidity and mortality. His initial ECG in the ED ( = E CG # 1 ) is shown in Figure-1.
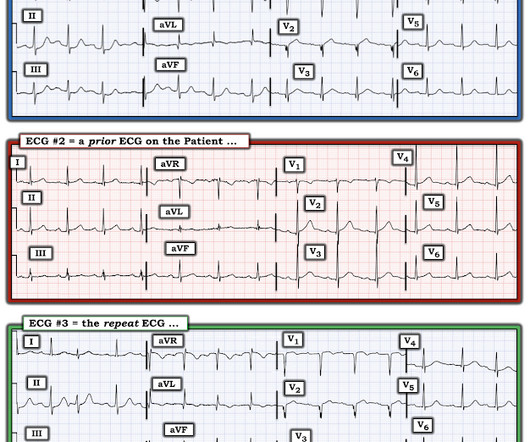
Here is the ED ECG: What do you think? The amiodarone was discontinued and the patient did well. == MY Comment , by K EN G RAUER, MD ( 6/23 /2023 ): == From an academic standpoint — I love WCT ( W ide- C omplex T achycardia ) rhythms. For clarity in Figure-1 — I've reproduced and labeled the 2 ECGs in today's case.
We discussed some practices to push learners outside of their comfort zone and promote learning, based on their level as well as their goals for the shift.
The overuse of computed tomographic (CT) scans for patients who present to the emergency department (ED) after mild traumatic brain injury (mTBI) has been well-documented. The Canadian Computed Tomography Head Rule (CCHR) is a validated tool to guide ED providers in determining the need for emergent CT of mTBI patients.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content