This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
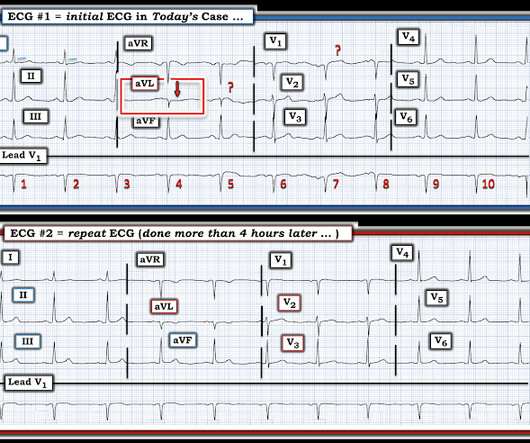
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. EKG on arrival to the ED is shown below: What do you think? Blood glucose was not low at 162 mg/dL.
All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes.
Authors: Adam Roussas, MD, MBA, MSE // Reviewed by: Jamie Santistevan, MD ( @jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD ( @MPrizzleER ); and Brit Long, MD ( @long_brit ) Case A 40-year-old female presents to the emergencydepartment for palpitations and lightheadedness. What do you do?
EKG, labs, and a CXR are interpreted by the EP as normal. An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. It wasn’t, so you weren’t called, nor did the doc need to document anything. This patient’s history was either poorly taken or poorly documented.
PI monitoring and treatment are often overlooked in the emergencydepartment (ED). Emergency care professionals must be proactive about PI early identification and prevention strategies. A team at a Level 1 trauma center recognized the need for ED-friendly documentation and a validated ED skin risk assessment instrument.
Her presenting EKG is shown below. The exact mechanisms by which these genetic mutations lead to the characteristic ECG and arrhythmias seen in Brugada Syndrome are not yet fully understood, but they are thought to involve abnormalities in cardiac ion channels that affect the flow of sodium and calcium ions across cardiac cell membranes 6.
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergencydepartment, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. See Ken Grauer's additional comments about this ECG at the end of the post!
During initial assessment, an ECG was obtained and revealed ST-segment elevation (STE) in the inferior leads with ST depression anteriorly. Initial ECG demonstrating inferolateral ST segment elevation and anteroseptal depression, just prior to cardiac arrest. The ECG showed ST-segment elevation without obstructive coronary disease.
While a randomized control trial should be done to evaluate the effect of early proning in a controlled environment, these studies suggest that we should consider using this in our EmergencyDepartment for patients who present with hypoxia and concern for mild to moderate ARDS without urgent need for intubation. Suction as needed.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. These diagnoses were not found in his medical records nor even a baseline ECG. The patient continued having chest pain.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. The following ECG was obtained.
Triage EKG: What do you think? A prior ECG was available for comparison. Prior EKG from 2 months ago was available: Let's put the precordial leads from the 2 ECGs side by side: Now you can really see the difference. Immediately after the second ECG was performed, the patient's pain resolved completely.
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
Duchenne Muscular Dystrophy (DMD) is a complex and progressive disease requiring highly specialized care, especially in emergency situations. When patients with DMD present in the EmergencyDepartment (ED), an understanding of the nuanced aspects of their care is essential for optimal management.
She presented to the emergencydepartment after a couple of days of chest discomfort. The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. How do you interpret the below ECG? This is very prolonged.
This month, after a few months of primarily medical topics, we’re talking trauma, specifically Blunt Cardiac Injury: EmergencyDepartment Diagnosis and Management. Post opiate hypotension in prehospital trauma patients is a rare but documented complication. New EKG findings requires admission for monitoring.
The overuse of computed tomographic (CT) scans for patients who present to the emergencydepartment (ED) after mild traumatic brain injury (mTBI) has been well-documented. The Canadian Computed Tomography Head Rule (CCHR) is a validated tool to guide ED providers in determining the need for emergent CT of mTBI patients.
Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. The remainder of his EmergencyDepartment stay was uneventful. His triage at 0127 is the ECG above. His triage at 0127 is the ECG above.
ECG, CXR, and troponin are negative. A medical student reports a murmur, not documented by either the emergency physician or the cardiologist. Troponins #1 and #2 are borderline and ECG is non-specific. In the ED, his troponin, ECG, and chest X-ray (CXR) are normal. ECG, CXR, and troponin are all normal.
Impact of intravenous calcium with diltiazem for atrial fibrillation/flutter in the emergencydepartment. Am J Emerg Med. What They Did: Researchers conducted a multicenter, retrospective cohort study in three community hospitals and two freestanding emergencydepartments. Article: Rossi N et al.
It was ongoing on arrival in the emergencydepartment. Below is the old ECG (on top) and then new ECG (on bottom). The old ECG has proportional ST elevation and T waves. So this STE cannot be considered normal even though there was STE on the previous ECG. But the ECG still doesn’t meet STEMI criteria.
to teach you and your learner something new on shift skin adhesives WITH dr. hill Dermabond is a polymer (octyl cyanoacrylate) that can be used to repair lacerations in the EmergencyDepartment faster than sutures, allowing the ED physician to be more efficient.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Here is the first ED ECG, with no pain: Sinus rhythm. It was stented.
This month, we are sticking in the abdomen for another round of evidence-based medicine, focusing on EmergencyDepartment Management of Patients With Complications of Bariatric Surgery. Vitamin D, B12, Calcium, foate, iron, and thiamine deficiencies are all well documented complications.
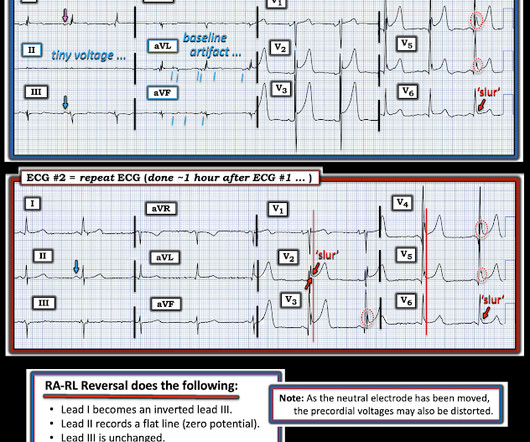
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergencydepartment (ED). It was immediately discerned that the patient had dextrocardia from previous records, and an EKG for dextrocardia was obtained.
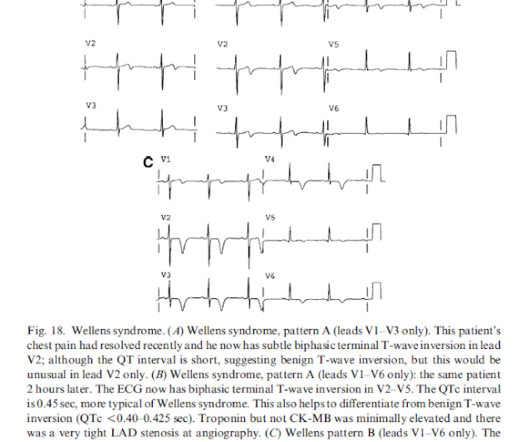
The pain resolved as he arrived to the emergencydepartment. Here was his triage ECG. This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. BP was 200/100.
52-year-old lady presents to the EmergencyDepartment with 2 hours of chest pain, palpitations & SOB. Here is her 12-Lead ECG: There’s a sinus rhythm at around 70 bpm. It is difficult to answer this question based on this single ECG alone. This was written by Sam Ghali ( @ EM_RESUS ), with a few edits by me.
Here is his initial ECG: 00:04 What do you think? With no other information other than the first ECG above, I texted this to Dr. Smith and he responded: ST elevation in lead V2 and terminal QRS distortion in V3. Therefore, this ECG would not have met the criteria for ACO by this formula. LAD occlusion. Great case.
Recently published experiments with LLMs in the emergencydepartment fall into a handful of primary areas of interest. In a similar vein, another study evaluated the ability of an LLM to assess “clinical acuity” in the emergencydepartment. J Am Coll Emerg Physicians Open. 2024;26(1):40-46. JAMA Netw Open.
However, evaluating and managing patients with acute alcohol intoxication in the emergencydepartment can be challenging. Document at each reassessment and always have a low threshold to add on a CTH or labs if the patient is not progressing appropriately. As always, document clinical sobriety before discharge.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. 1,4-5 Thus, an electrocardiogram (ECG) and cardiac monitoring should be performed for unstable, electrical injury patients.
Emergency physicians have earned the right to “re-brand” ourselves as indispensable, money-saving change agents in the health care enterprise. Of course, the bill for any episode of emergencydepartment (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices.
A 59-year-old man presents to your community emergencydepartment (ED) with chest pain that is radiating to his back. His vital signs are normal and the ECG does not demonstrate a myocardial infarction. Emerg Med Australas. Your clinical gestalt has you suspecting an acute aortic dissection (AoD). 2018;30:119–21.
Written by Destiny Folk MD, with edits by Meyers, peer reviewed by Smith and Grauer A woman in her late 20s with a past medical history of cervical cancer status post chemotherapy and radiation therapy presented to the emergencydepartment for shortness of breath, chest tightness, and two episodes of syncope.
Jeff: Abdominal pain is the one of most frequent complaint in US emergencydepartments, representing 8% of all adult ED visits, with admission rates for all patients with abdominal pain ranging between 18-42% and reaching as high as 60% for the elderly. Nachi: And finally let’s touch upon the ekg and ACS. Jeff: True. Review) 83.
Abnormal ECG – looks for cardiac syncope. Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. If no previous ECG was available, ECG was classified as abnormal if any abnormality was present. orthostatic vitals b.
Here’s the paramedic ECG (digitized by PMcardio). I sent the ECG to Dr. Meyers without any information, and he immediately replied, “inferior OMI.” Here’s the first and repeat paramedic ECG: According to some interpretations of the literature on “transient STEMI”, this patient doesn’t need the cath lab because ST segments improved.
I see one patient at a time, and I document after each patient. Picking up multiple patients at once and postponing documentation seems like it would make you faster, but mostly it just makes you less effective. In most environments, an important goal of documentation is billing. Review at the vital signs. Write your note.
This was submitted by Hans Helseth, who is applying to med school and who is working as an EKG tech right now. He looked back in time in the patient's chart and saw these ECGs and immediately recognized that they manifested subtle OMI. He had an EKG recorded right away. EKG 1, 1646: What do you think?
then need further evaluation Usually with CTA imaging If normal physical exam & ABI>0.9, million presentation to ED’s throughout the US Usually occur due to falls Also commonly occur due to sports, MVC’s, etc.
She presented to the EmergencyDepartment at around 3.5 Here is her triage ECG: What do you think? The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR).
Work-up and Diagnosis in the EmergencyDepartment Initial presentation of TLS typically includes generalized symptoms such as gastrointestinal distress, decreased appetite, muscle cramping, palpitations, hematuria / oliguria, and altered mental status. original document created by author of post. in females and 2.5-7.0
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content