This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A young man presented with a gunshot wound to the right chest, with hemo-pneumothorax and hemorrhagic shock. I’ve attached an article and an abstract (that article is in Japanese unfortunately … ) that do document that you CAN however on occasion find AIVR in otherwise healthy children — and I suppose that IS what we have here.
Figure-2: I've color-coded P waves from Figure-1 according to P wave morphology ( See text ). NOTE: For clarity — I've color-coded P waves in the long lead II rhythm strip according to morphology. MAT almost always occurs in one of 2 common predisposing settings.
Read the document for all the details (it’s not long). three shocks with 2 minutes CPR in between) have been performed. In accordance with the fraught ethical and emotional factors surrounding organ donation, this section is the tersest, least explicated section of the document. Cooling patients to targets below 37.5°C
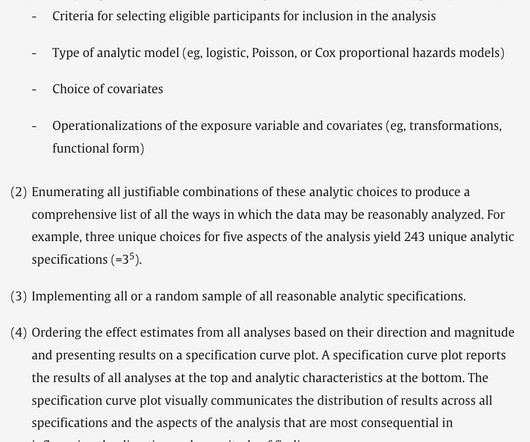
This came as a shock to me. In this section, they documented the variations in analytic method (for instance, the choice of model and co-variates). The cardiac literature overflows with association studies, but each one uses one analytic method. What if different scientists chose to analyze the data in different ways.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated.
Shocked x 2 without effect. Warning: if this is VT, a calcium channel blocker can result in shock and death. Today's case is insightful in many ways — especially since despite prompt electrical cardioversion, we are told that this patient "was shocked X 2 without effect". However, this is not SVT. What to do now? K returned 3.6
is to restrict caloric delivery in patients with this degree of shock. To make that leap, I for one would need to see improved outcomes with caloric restriction in patients with less-severe shock. Computers writing progress notes holds huge potential for reducing the 50% of working hours time doctors spend documenting.
Current SSC guidelines recommend fluid resuscitation with at least 30mL/kg IV crystalloid in patients with sepsis induced hypoperfusion or septic shock within the first three hours of resuscitation, regardless of comorbidities. Evaluation and Predictors of Fluid Resuscitation in Patients With Severe Sepsis and Septic Shock.
Sodium Chloride or Hartmanns if indicated, monitoring for signs of shock. Provide detailed documentation of the initial assessment, treatment provided, and the patient’s response to interventions. Establish IV access and begin fluid resuscitation with 250ml boluses of 0.9% Check temperature and blood glucose levels.
Get a blood gas when possible to help guide your ventilation. glenn, haffner, and jackson In Flight Emergencies: As a responding physician to an in-flight emergency, you may recommend diverting the plane, however, the captain (lead pilot) will make the final decision.
Nontraumatic hypotension and shock in the emergency department and the prehospital setting, prevalence, etiology, and mortality: a systematic review. Emergency department hypotension predicts sudden unexpected in-hospital mortality: a prospective cohort study. 2006;130(4):941–6. PMID: 17035422 Holler JG, et al. 2015;10(3):e0119331.
See screenshot: The endpoint was the proportion of patients whose chart had a documented goals of care care discussion. In a university hospital system known for its strength in palliative care, only a third of seriously ill patients in the intervention arm have a documented goals of care discussion. The absolute risk difference of 4.1%
A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chest pain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. KEY Point: The respiratory rate that is written on the chart does not count!
For anyone approaching a structured ABC would be a priority to establish whether shock was present or not. Typical features include: HR >220bpm Narrow complex regular tachycardia P waves difficult to identify In this case there is no shock present so we can proceed to the right branch of the ALSG guideline.
Quick Shock Delivery and Fast Charging In a life-threatening situation, quick response time is vital. Philips defibrillators are designed to deliver a shock quickly, minimizing the time between chest compressions and defibrillation. This rapid shock delivery feature can significantly improve the chances of a successful resuscitation.
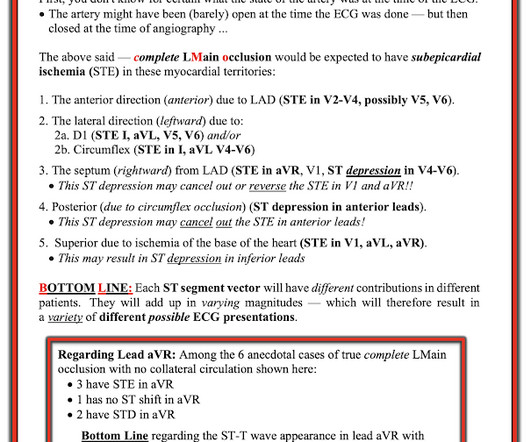
The patient in today’s case presented in cardiogenic shock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. In both tracings — an exceedingly fast PMVT is documented. LAD — 100% proximal occlusion; with 70-89% mid-vessel narrowing. RCA — 100% proximal occlussion.
of patients with follow-up documentation, 70.8% (95% CI 62.9–77.9) Data collected were the worst values documented within the same calendar day as the blood cultures were obtained. Outcomes included clinical status when urine culture was available, subsequent antibiotic treatment within seven days and subsequent UTI within 30 days.
She was in shock with thready pulses. The rate is not fast enough to be causing shock, so if it is VT, the priority is still to treat hyperK and secondarily to cardiovert. They thought it was VT, but did not shock. On arrival, the patient was in shock, was intubated, and had an immediate cardiac ultrasound.
Their AEDs are designed to be user-friendly, reliable, and effective in delivering life-saving shocks to restore a normal heart rhythm. Escalating Energy : This feature allows the AED to automatically increase the energy level of subsequent shocks if the initial shock is unsuccessful, increasing the chances of restoring a normal heart rhythm.
What They Did: Double-blind, randomized, placebo controlled trial that ran from October 2019 through January 2024 Multinational study conducted at 22 centers in three European countries 3512 patients were enrolled and before surgery eligible patients were randomly assigned to one of the following two groups Amino Acid Group: 10% Isopuramin at a dose (..)
Epi vs. NorEpi Spoon feed: Continuous epinephrine infusion for post-resuscitation shock in out of hospital cardiac arrest (OHCA) was associated with both higher all-cause and cardiovascular specific mortality when compared to norepinephrine. Check out journalfeed.org for details.
Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. This segues relatively nicely into a section of the document on palliative care. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. To start with there are apparently 5 types of cardiorenal syndrome.
While patients received respiratory support, supportive care, and antibiotics at the discretion of the medical team, the specific interventions provided outside the study were not documented, potentially leading to co-intervention bias. More than 75% of patients did not complete the treatment course.
This month, we’ll be talking Updates and Controversies in the Early Management of Sepsis and Septic Shock. And sepsis-3 redefined septic shock as “hypotension not responsive to fluid resuscitation” with the added requirement of vasopressors to maintain a MAP greater than or equal to 65 and with a lactate > 2. That’s where we’re at.
Unlike vehicles, bicycles have less stability and shock absorption, making them more susceptible to road imperfections. This documentation is vital for any subsequent legal proceedings and helps establish a clear record of the event. Moreover, these issues often go unrepaired for extended periods, exacerbating the risk.
Individualize the choice of using inotropes, vasopressors, or fluids to treat post-CA hypotension and to target the likely cause(s) contributing to the shock and hemodynamic state (100%, 23/23). In patients with enteral intolerance or shock, start with trophic EN (rates of 10–20 mL/h) and adjust according to tolerance (91%, 19/21).
There are two main reasons for an elevated lactate: the stress state and the shock state. The shock state is due to tissue hypoxia, seen in septic shock. We should use lactate to detect occult shock. Children compensate so well for shock, that subtle tissue hypoxia may not be detected until later. Am J Cardiol.
By delivering an electric shock to restore normal heart rhythm in cases of ventricular fibrillation or other arrhythmias, AEDs play a vital role in increasing survival rates following sudden cardiac arrests. If it detects such a problem, it delivers an electric shock to restore normal heart function.
He had no previously documented medical problems except polysubstance use. below) Other examples of AIVR: Young man with Gunshot wound to right chest with hemorrhagic shock, but bullet path not near heart. He reported a history of “Wolf-Parkinson-White” and “heart attack” but said neither had been treated. Leave it alone. Bigger et al.
A 200J shock is reasonable – though a higher dose may be needed for larger patients. The literature base for the use of lidocaine for torsade storm is documented primarily by case studies in drug-induced TdP. Assess your patient and if there is any sign of instability, use electricity.
Keep Track of Maintenance and Servicing Proper documentation of maintenance and servicing activities is crucial for record-keeping and compliance purposes. Expired pads or batteries may not deliver the shocks or power required in a life-saving situation.
Don’t forget the essentials: Eat Hydrate +/- caffeinate Exercise Unwind Sleep It’s not rocket science, but it’s shocking how many of us forget! Don’t be afraid to ask the simple questions: Where do I document? Top tip: verbally communicating your plan followed by clear documentation can help avoid confusion!
This does not mean that all patients need to be immediately shocked — but it does mean that since 90+% of such rhythms will turn out to be VT, that we need to assume VT until proven otherwise. Because of this 1st bullet — We need to always assume VT for such rhythms until we prove otherwise, and treat accordingly.
4 Using factors such as shock, pneumonia, and sepsis this score allows an accurate prediction of developing ARDS. There may have very well been a policy where only RTs can make changes to a ventilator after an order was placed to ensure accurate documentation.
saline vs balanced crystalloid solutions for initial fluid management in the treatment of septic shock which may give us more insight into this topic. [5] They concluded that some evidence in the literature shows a shorter length of hospital stay associated with prescribing balanced isotonic fluids (Plasma-lyte) over non-balanced (0.9%
Trauma patients between the ages of 18-90 years had to have either had one documented episode of hypotension (defined as a systolic BP <90 mmHg) or tachycardia (>100 beats/minute) to be included in the study. When looking at the subgroups with severe shock, there was an 18.5% MI or stroke).
Electrical injuries—excluding lightning injuries—account for roughly 10,000 nonfatal shock incidents a year and 500 deaths a year. Documentation with coronary arteriography within 12 1/2 hours of the onset of symptoms in two cases (three episodes). FIGURE 2: Traumatic amputation and electrical burn of the patient’s left arm.
Essentially there was no difference, meaning we wouldn’t expect to find a difference in outcomes Although not patient oriented, why is there no breakdown of how many patients had cardiogenic shock, congestive heart failure, echocardiographic findings, or even troponin levels. Low O2 protocol: 3.1% aOR 0.96, 95% CI 0.86 Low O2 protocol: 10.6%
The others, such as respiratory rate, heart rate, and decompensated shock, were excluded due to the presumed difficulty for non-healthcare professionals to assess them accurately. Inclusion criteria required documented acute streptococcal pharyngitis, as per positive throat swab culture or rapid antigen testing, in patients 1-18 years of age.
Documents improvements in BVMs previously investigated and found deficient in FIO2. Classic pre-EMS document describing rescue care by rural volunteer squads. Committee on Shock. **Critical exam of poor FIO2 delivery, valve-jamming, rebreathing, reservoir designs. CARDEN, E., & FRIEDMAN, D. Abdo Khoury, M. Hugonnot, S.,
The next job is to document clearance from the blood. There are some nuances once you get into the weeds (and beyond the scope of an ICU exam) about addition of aminoglycosides (not routinely recommended) or addition of rifampicin (generally only in the context of prosthetic joints or hardware). once on the bug juice repeat the cultures.
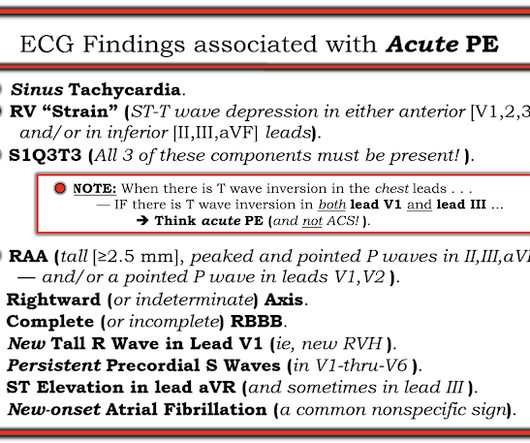
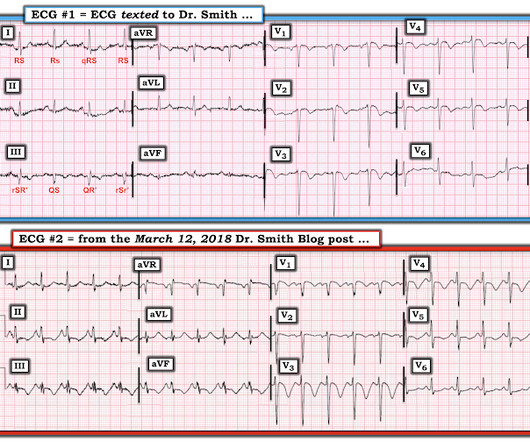
Tachycardia is unusual in ACS unless there is cardiogenic shock or a second simultaneous pathology. Finally — Note that the S1Q3T3 pattern is missing in ECG #2 , despite documentation of a massive PE. Remember that is the odds ratio comparing all patients without PE to those with PE.
Perhaps, not insignificantly, they were accustomed to receiving systematized government-supplied medical and trauma care, with "shock rooms" receiving an influx of victims, as contrasted to those later who opposed "socialized medicine." Committee on Shock. EMS in America: The Foundation Documents. Sakran, J.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content