emDOCs Podcast – Episode 98: Post ROSC Mental Model
EMDocs
APRIL 2, 2024
Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model in post ROSC patients. Episode 98: Post ROSC Mental Model What’s the problem?
 CPR EKG/ECG Ultrasounds
CPR EKG/ECG Ultrasounds 
EMDocs
APRIL 2, 2024
Today on the emDOCs cast Brit Long interviews Zachary Aust on the use of a mental model in post ROSC patients. Episode 98: Post ROSC Mental Model What’s the problem?
ACEP Now
JANUARY 4, 2025
A closer look, though, also shows the technology of the daya bulky, two-way radio for communicating with EMS, metal gurneys, glass saline bottles, and portable ECG monitors the size of a small shopping cart. Notice the use of the medical anti-shock trousers and the ECG machine. Now, we have ultrasound or CT scans to confirm.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.

Dr. Smith's ECG Blog
APRIL 2, 2024
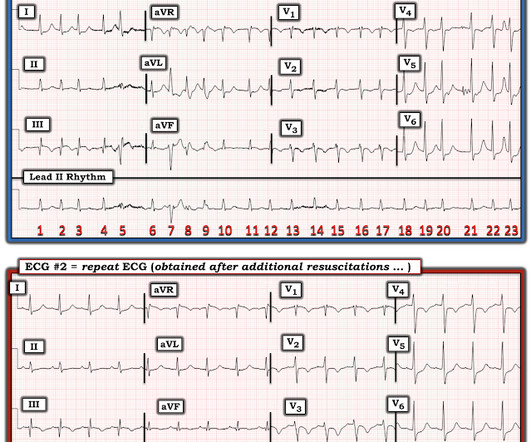
There was no bystander CPR. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. Another ECG was recorded 12 minutes later: Paced rhythm, probable Pacemaker-Mediated Tachycardia ?

Dr. Smith's ECG Blog
MAY 19, 2020
ECMO Flow was achieved after approximately 1 hour of high quality CPR. A followup ECG was recorded 2 days later: No definite evidence of infarction. The ways to tell for certain include intravascular ultrasound (to look for extra-luminal plaque with rupture) or "optical coherence tomography," something I am entirely unfamiliar with.

The Skeptics' Guide to EM
SEPTEMBER 11, 2021
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. The EKG shows sinus tachycardia with nonspecific changes and no ST segment elevations, Q waves, or hyperacute T waves. The AHA has a statement with recommendations based on the available data.
Dr. Smith's ECG Blog
OCTOBER 24, 2013
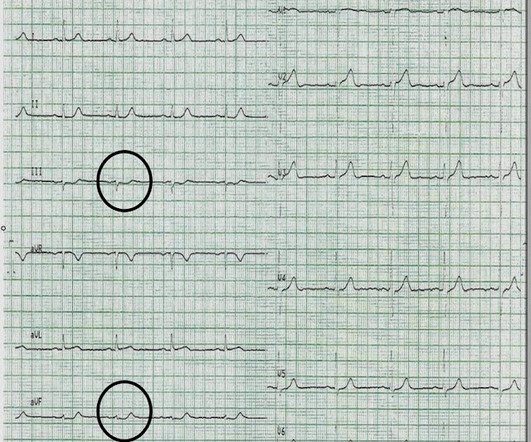
The physician recorded this ECG, interpreted it as normal, and sent the patient home on an antacid. He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. I do not have the post-resuscitation ECG. Did the ECG offer unseen hints? See explanation below. Lesson : 1.

Dr. Smith's ECG Blog
NOVEMBER 30, 2019
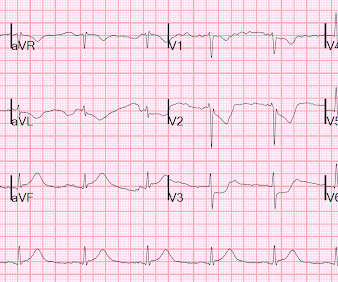
A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy? On arrival, the patient was in shock, was intubated, and had an immediate cardiac ultrasound. What does a heart look like on ultrasound when the EKG looks like that? The followup ECG is here: Now the QRS is only slightly prolonged.

Expert insights. Personalized for you.













Let's personalize your content