
Ultrasound in Cardiac Arrest
Mount Sinai EM
AUGUST 7, 2024
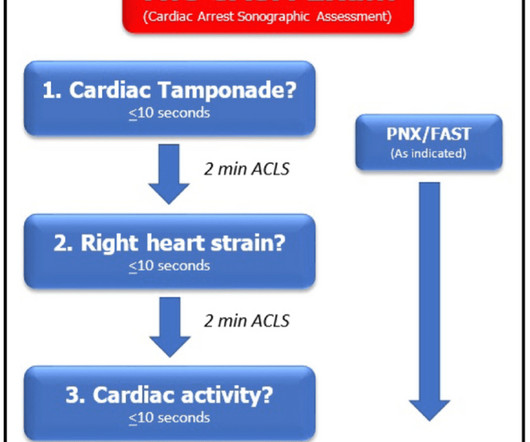
Ultrasound during cardiac arrest has quickly become standard. Initially, data suggested that the use of ultrasound during arrest increased pauses between compressions which worsens outcomes. Finally, patients with PEA and cardiac standstill on ultrasound have a 0.0%-0.6% Yours in ultrasounding, Shivam















Let's personalize your content