This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These 2 settings are: i ) In patients with severe , often longstanding pulmonary disease ; and / or , ii ) In acutely ill patients with multi-system disease ( ie, sepsis, shock, electrolyte and/or acid-base disorders ). Applying the Above to Today's Case: In addition to being Covid-positive — the patient in today's case had longstanding COPD.
It can be used to distinguish between various conditions, including chronic obstructive pulmonary disease (COPD) exacerbation, acute heart failure (AHF), pleural effusion, pulmonary edema, pericardial effusion, pneumothorax, and pneumonia [2,3]. thus prolonging their hospital stay and increasing readmission rates.
This month, we’ll be talking Updates and Controversies in the Early Management of Sepsis and Septic Shock. For those listening, my hospital probably looks a little bit like yours. Roughly half of in-hospital mortality is associated with septic in some fashion. At our hospital in northern Manhattan they like to breath around 18.
It can be further divided into two types: primary--those that occur in generally healthy individuals without underlying lung disease, and secondary--those that occur in individuals with underlying lung disease such as COPD [1]. Smoking is a known risk factor, as is cannabis use [2,5, 7-8].
1-3 VTE is responsible for hospitalizing over 250,000 Americans every year, and there are an estimated 100,000 deaths annually associated with these conditions. However, as shock resolved and hemodynamic stability improved, RV strain and underfilling of the LV remained apparent 30 minutes after ROSC (Vid 4). 10,11 Vid 1.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Given her tachycardia and episodes of syncope, the patient was judged to be in compensated obstructive shock with very high risk of imminent decompensation. She was discharged after a short hospitalization with oncology and cardiology follow-up. Fluid samples were sent for culture and cytology and results showed malignant cells.
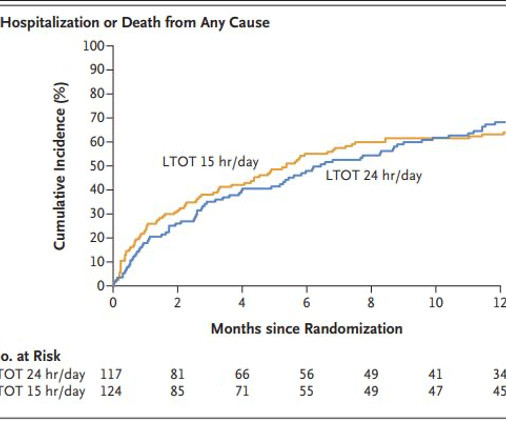
In studies, and in practice, these people tend to be patients with COPD who have resting O 2 sats of < 88%. The primary outcome was a composite of hospitalization or death from any cause within one year. About 80% had either COPD or pulmonary fibrosis and the mean PaO 2 and O 2 sats were about 50mm Hg and 80%, respectively.
Authors: Rachel Kelly, MD ( EM Resident Physician, Stony Brook University Hospital); Robert Nocito, MD (EM Attending Physician, Stony Brook University Hospital) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University in St. is more likely to portend death (13, 14).
Follow your hospital’s protocol (if available). High Risk Patients will need hospitalization and IV antibiotics. Give appropriate fluids, vasopressors, and antibiotics. This will have been formulated based on local resistance patterns and likely with input from your institution’s oncologists.
Four days ago, he presented to the ED for a COPD exacerbation. On chart review, a sputum culture collected during a recent hospital visit grew a species of Aspergillus. COPD, cystic fibrosis), HIV/AIDS, cancer, immunosuppressed (i.e. COPD, cystic fibrosis), HIV/AIDS, cancer, immunosuppressed (i.e.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content