This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
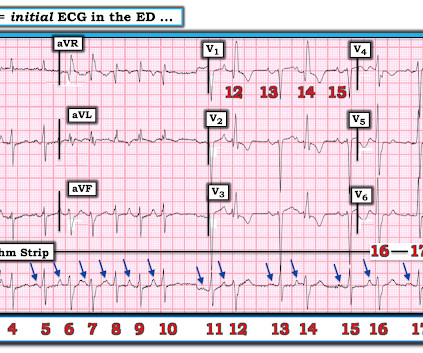
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chest pain. Here is the ECG: What do you think? Shah and Rubin studied the computer rhythm interpretation of 2160 12-lead ECGs, compared to 2 cardiologists [ 18 ]. noted computer over-interpretation (false positives) of AF in 9 to 19% of ECGs [ 19 ].
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. An immediate 12-lead EKG was obtained: There is ST elevation in leads aVR and V1, with marked ST depression in I, II, III, aVF, V3-V6. What should be done?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content