

ECG Blog #366 — Diltiazem didn't work.
Ken Grauer, MD
FEBRUARY 28, 2023
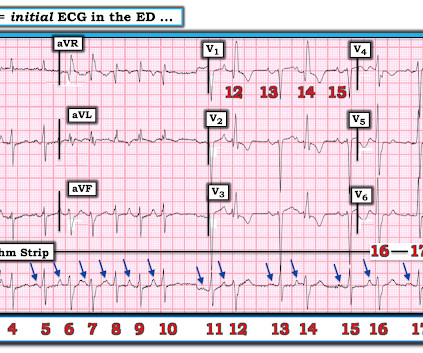
Figure-2: I've color-coded P waves from Figure-1 according to P wave morphology ( See text ). NOTE: For clarity — I've color-coded P waves in the long lead II rhythm strip according to morphology. Applying the Above to Today's Case: In addition to being Covid-positive — the patient in today's case had longstanding COPD.











Let's personalize your content