This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG in Figure-1 — was obtained from a middle-aged man with palpitations and shortness of breath. How would YOU interpret the ECG in Figure-1 ? Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). Figure-1: The initial ECG in today's case. (
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiac arrest. ROSC ( R eturn O f S pontaneous C irculation ) was obtained — and ECG #1 was recorded. In view of this history — How would YOU interpret the ECG in Figure-1 ? Should you activate the cath lab?
QUESTION: HOW would YOU interpret the ECG in Figure-1 — if no clinical information was provided? Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). = The ECG in Figure-1 — was obtained following successful resuscitation.
The ECG in Figure-1 was obtained from a man in his 40s — who presented to the ED ( E mergency D epartment ) because of CP ( C hest P ain ) and shortness of breath. QUESTIONS: In view of the above history — How would YOU interpret the ECG in Figure-1 ? Based on the history and the patient's initial ECG — the cath lab was activated.
I recently recorded a series of 4 podcasts regarding KEY concepts in ECG interpretation. Easy LINKS — tinyurl.com/KG-ECG-Podcasts — [link] — Other ECG Audio PEARLS I previously made for my ECG Blog can be found in the right column of each page on this blog just below this icon — under, "ECG Audio PEARLS".
The ECG in Figure-1 — was obtained from a patient with palpitations. Figure-1: The initial ECG in today's case. My Interpretation of the ECG in Figure-1: Since the patient is hemodynamically stable — there is time for systematic assessment of the rhythm. Figure-2: I've labeled the initial ECG in today's case. Figure-2 ).
The ECG in Figure-1 was obtained following successful resuscitation. QUESTIONS: In view of the above history — How would YOU interpret the ECG in Figure-1 ? Is this ECG finding present in today’s initial ECG? Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiac arrest. (
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiac arrest. How would YOU interpret her post-resuscitation ECG? Does this ECG in Figure-1 provide clue(s) to the etiology of this patient's cardiac arrest? QUESTIONS: In light of the above clinical history.
The ECG in Figure-1 — was obtained from an older woman with persistent CP ( C hest P ain ) over the previous day. Figure-1: The initial ECG in today's case. Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ).
She had an ECG recorded: This is left bundle branch block (LBBB), with appropriate proportional discordance. Here is one of the strips This is clearly polymorphic VT and probably torsade de pointes Subsequent ECGs. CT of the chest showed no pulmonary embolism but bibasilar infiltrates. but potassium returned normal. J Am Coll Cardiol.
MY Approach to the Rhythm in Figure-1: As per ECG Blog #185 — I favor the P s, Q s, 3 R Approach for interpretation of the cardiac rhythm — beginning with whichever of these 5 KEY Parameters is easiest to assess for the tracing in front of me: At least in the single lead II rhythm strip seen in Figure-1 — The Q RS complex appears to be narrow.
The ECG in Figure-1 is from an older man with known coronary disease — who presents to the ED ( E mergency D epartment ) with new CP ( C hest P ain ) over the past several days. QUESTIONS: In view of this history — How would you interpret the ECG in Figure-1 ? Figure-1: The initial ECG in today's case. Troponin is pending.
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. QUESTIONS: How would YOU interpret the ECG in Figure-1 ? Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). What is the differential diagnosis?
It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. The patient arrived just after 10 AM, and the following EKG was obtained. There are no further EKGs or troponin measurements.
1,2 Neuroleptic malignant syndrome (NMS) (hyperthermia, autonomic instability, rigidity, altered mental status [AMS]) can occur as well and is most often seen with clozapine but has been observed with other atypicals. 1,2 Cardiovascular: Obtain an initial EKG to determine the patient’s baseline and repeat. Published 2023.
The ECG in Figure-1 was obtained from an elderly woman — who presented to the ED ( E mergency D epartment ) for dyspnea on exertion over recent weeks. Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). What are YOUR "Quick Thoughts" about this case?
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. If this EKG were handed to you to screen from triage without any clinical information, what would you think? Do you appreciate any dynamic changes compared to the patient’s prior EKG? What do you think? In fact, Kosuge et al.
You are given this ECG to review. QUESTION: Is there a potential problem with this ECG? Figure-1: The initial ECG in today's case. == N OTE : Many of us are charged with reviewing ECGs that have been interpreted by other clinicians — often without the benefit of much ( or any ) history. The rhythm in ECG #1 is sinus.
The patient whose initial ECG is shown in Figure-1 — is a middle-aged man who presented to the ED ( E mergency D epartment ) for new-onset CP ( C hest P ain ). QUESTIONS: In view of the above history — How would YOU interpret the initial ECG? WHY is it important to correlate severity of this patient’s CP with ECG #1 ?
The ECG in Figure-1 was obtained from a man in his mid-60s — who presented with new chest pain. Figure-1: T he initial ECG in today’s case. MY Thoughts on the Initial ECG: The rhythm in ECG #1 — is sinus at ~70/minute. Figure-2: I've labeled significant ST-T wave findings in the limb leads of ECG #1.
The ECG in Figure-1 is from a man in his 30s — who overall has been healthy, except for a history of "intermittent palpitations" that he has had since childhood. He was hemodynamically stable with ECG #1. Figure-1: The initial ECG in today's case. To improve visualization — I've digitized the original ECG using PMcardio ).
The ECG in Figure-1 was obtained from an elderly man with a history of coronary disease — who contacted EMS for "burning" chest discomfort that woke him at 3am. Some amount of time passed at home — during which his chest discomfort persisted The patient was hemodynamically stable at the time he was seen by EMS, when ECG #1 was recorded.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
I start today’s case with the ECG shown in Figure-1 — obtained from a 30-something year old man, who presented with palpitations. How would YOU interpret the ECG in Figure-1 ? Figure-1: The initial ECG in today’s case. To improve visualization — I've digitized the original ECG using PMcardio ). What is the rhythm?
He was not symptomatic with the ECG shown in Figure-1. How would YOU interpret this ECG? Extra Credit ( which is a HINT to the Answer! ): How many beats are recorded on the ECG in Figure-1 ? Figure-1: The initial ECG in today’s case. ( To improve visualization — I've digitized the original ECG using PMcardio ).
T he ECG in Figure-1 was obtained from a 60ish year old man on arrival to the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case — obtained from a 60ish year old man who collapsed in the ED shortly after this tracing was recorded. ( To improve visualization — I've digitized the original ECG using PMcardio ).
The ECG in Figure-1 was obtained from a previously healthy 30-ish year old man — who presented to medical attention for vasovagal syncope. Based on this initial ECG — the patient was transferred to a PCI-capable center: Do YOU agree with the need for transfer? Figure-1: The initial ECG in today's case.
The 12-lead ECG and long lead rhythm strip in Figure-1 — was obtained from a previously healthy 15-year old male , who presented with fever and diarrhea. How would YOU interpret the ECG in Figure-1 ? Figure-1: The initial ECG in today’s case — obtained from a 15-year old male with fever and diarrhea. No chest pain.
This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. This EKG is very subtle, but it is diagnostic of LAD occlusion. The Queen of Hearts does not see the hyperacute T waves.
speed that many of us are used to ) — BUT — that the width of each large box on the ECG grid paper has been reduced by 50% ( so that each small rectangular box on this ECG grid paper still represents 200 msec. = R-R interval for the first few beats in this tracing ). == H ow M any P - W aves are there in ECG Rhythm #1?
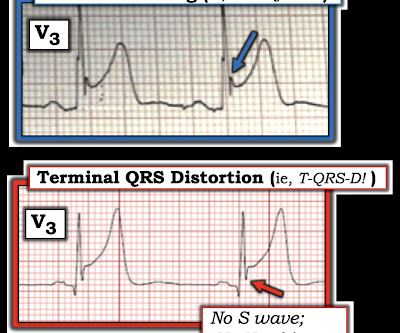
He had active chest pain at the time of triage at 0137 at night, with this triage ECG: What do you think? I sent this ECG, without any text at all, to Dr. Smith, and he replied: "LAD OMI with low certainty. Back to the case: Unfortunately, the ECG was not understood by the provider. V3 is the one that is convincing."
Written by Pendell Meyers Try first to interpret the ECG without any clinical context: What do you think? Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. There was no prior ECG for comparison. To improve visualization — I've digitized the original ECG using PMcardio ).
I said, "Cool, can I see the ECG?' So he showed me the ECG recorded in triage: What did I say? Then he said: "No wonder the next EKG we recorded just before she left for the cath lab was normal." I came to work one day and one of my partners said, "Hey, Steve, we had a STEMI this afternoon!" That is not a STEMI. He said: "What?
I have often written about how an ECG interpreted as "normal" by a conventional algorithm may well be manifesting OMI, or even long QT or hyperkalemia. Shifa Karim and Gabe Keller helped with a project to assess all these ECGs with the Queen of Hearts. The ECG told the story. I wanted to show some of the cases here.
Below is the triage ECG, with a computer interpretation (Marquette 12 SL) of “normal” which was confirmed by the over-reading cardiologist. Should this patient continue to stay in the waiting room, without interruption of the physician to interpret the ECG, because the computer interpretation is normal? What do you think?
Written by Pendell Meyers First try to interpret this ECG with no clinical context: The ECG shows an irregularly irregular rhythm, therefore almost certainly atrial fibrillation. Here is the initial ECG: A temperature sensing Foley was inserted and reported a core temperature of 26.7 He did well and was discharged.
A 50 year old presented to the emergency department of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. What do you think, and how would you manage the patient? The Need for Immediate Transport?
This is the result for this ECG, from MDcalc.com : The most accurate cutpoint is 18.2. And she learned it well: She is not highly confident, but she does diagnose OMI. Here is a similar case from Pendell: This ECG was handed over at triage. A value above 18.2 (LAD A value above 19 is about 97% specific for LAD OMI.
An ECG was recorded immediately and is shown below. How do you interpret the ECG? ECG#1 There is a regular tachycardia with a ventricular rate of about 180 bpm. After cardioversion, if successful, you can take a few moments to assess the 12-lead in more detail and assess the post conversion ECG. ECG#2 What do you think?
This ECG was texted to me with no other information. The first ECG was recorded at 53 minutes after pain onset. The pain began to improve and this ECG was recorded: T-waves are not quite as tall, though still have a large AUC. An old ECG was found: As you can see, this patient has zero baseline STE, and normal T-waves.
Below is old and then new ECG (old on top; new below). Both ECGs have normal sinus rhythm, normal conduction and normal voltages. Because of the ECG changes in a patient with chest pain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. What do you think? But do they represent acute coronary occlusion?
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( Chest Pain ). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation. For 2 of the 3 patients — the cath lab was activated based on the ECG.
The following ECG was obtained. ECG 1 What do you think? The ECG shows sinus bradycardia but is otherwise normal. There is TWI in lead III, but this can be seen in normal ECGs. The following ECG was obtained around midnight. The machine read was "Normal sinus rhythm, normal ECG." ECG 2 What do you think?
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" On arrival to the ED, while waiting for cath lab team, he obtained another ECG: You can now see the full voltage of the high-voltage QRS, likely with some degree of LVH. Serial ECGs remained unchanged. But he did well.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content