This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
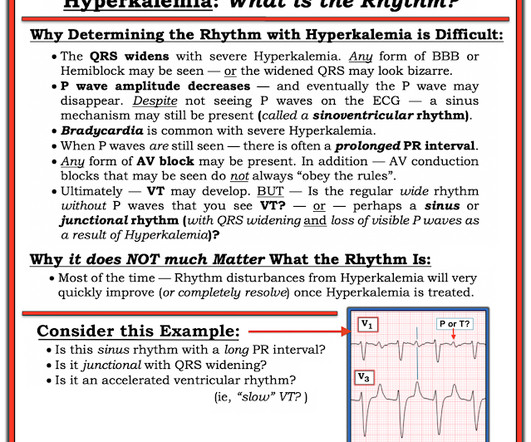
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiac arrest. How would YOU interpret her post-resuscitation ECG? Does this ECG in Figure-1 provide clue(s) to the etiology of this patient's cardiac arrest? QUESTIONS: In light of the above clinical history.
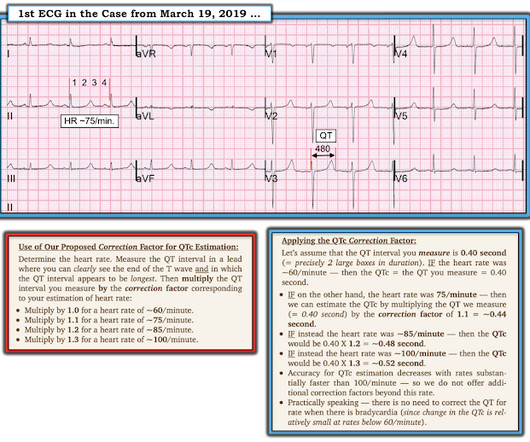
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( To improve visualization — I've digitized the original ECG using PMcardio ).
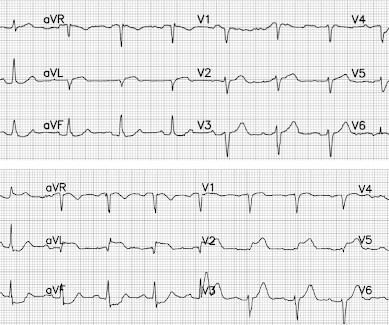
She had an ECG recorded: This is left bundle branch block (LBBB), with appropriate proportional discordance. In the middle of the night, a "code" was called, and multiple rhythms like this were recorded. Here is one of the strips This is clearly polymorphic VT and probably torsade de pointes Subsequent ECGs. J Am Coll Cardiol.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. If this EKG were handed to you to screen from triage without any clinical information, what would you think? Do you appreciate any dynamic changes compared to the patient’s prior EKG? What do you think? In fact, Kosuge et al.
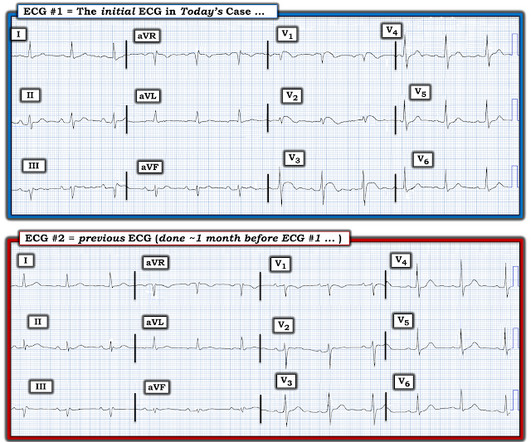
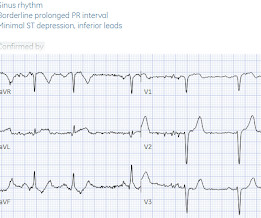
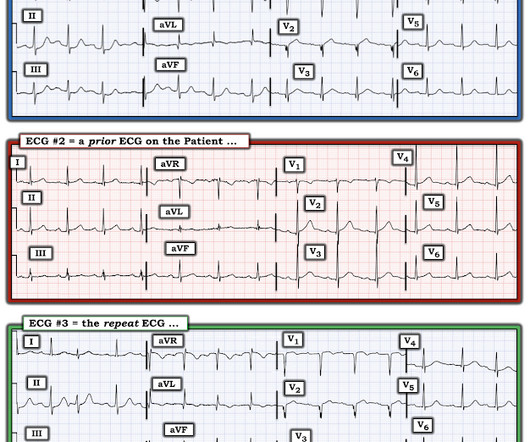
Below is old and then new ECG (old on top; new below). Both ECGs have normal sinus rhythm, normal conduction and normal voltages. Because of the ECG changes in a patient with chest pain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. What do you think? But do they represent acute coronary occlusion?
What do you think of the ECG, and does it matter? I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. 2] This is because, contrary to Bayesian reasoning, the STEMI paradigm is named after and defined by one part of one test: ST elevation on ECG. But only 6.4%
All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes.
I have often written about how an ECG interpreted as "normal" by a conventional algorithm may well be manifesting OMI, or even long QT or hyperkalemia. Shifa Karim and Gabe Keller helped with a project to assess all these ECGs with the Queen of Hearts. The ECG told the story. I wanted to show some of the cases here.
Willy is a cardiology fellow with a keen interest in the ECG in OMI. Triage documented a complaint of left shoulder pain. If an immediate EKG was obtained, it was not saved in the medical record. A patient with OMI can have a totally normal ECG!" Cardiology was consulted, and repeat EKG was obtained at around 2:30 AM.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chest pain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. see reference below) Whats the gold standard for ECG interpretation: is it cardiologist interpretation? What do you think? The latest is Langlois-Carbonneau et al.
Below is the triage ECG, with a computer interpretation (Marquette 12 SL) of “normal” which was confirmed by the over-reading cardiologist. Should this patient continue to stay in the waiting room, without interruption of the physician to interpret the ECG, because the computer interpretation is normal? What do you think?
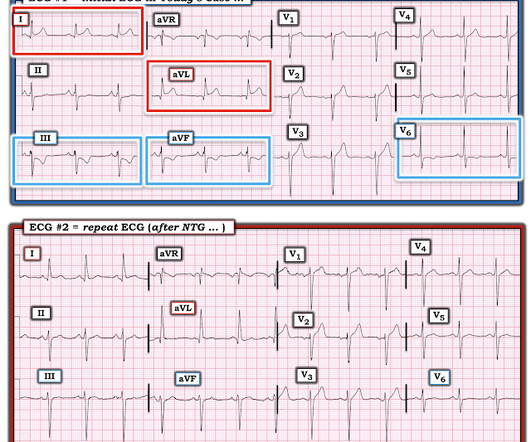
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He had a previous ECG on file: Proving the findings are new The cath lab was activated. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. No other symptoms.
The documentation does not describe any additional details of the history. The following ECG was obtained. ECG 1 What do you think? The ECG shows sinus bradycardia but is otherwise normal. There is TWI in lead III, but this can be seen in normal ECGs. The following ECG was obtained around midnight.
This ECG was texted to me with no other information. The first ECG was recorded at 53 minutes after pain onset. The pain began to improve and this ECG was recorded: T-waves are not quite as tall, though still have a large AUC. An old ECG was found: As you can see, this patient has zero baseline STE, and normal T-waves.
Here is the ECG: Computer interpretation: Normal ECG Interventionalist after doing PCI: SUBTLE STT CHANGES IN LIMB LEADS To me, this first ECG is diagnostic of inferior OMI. I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: YOU TOO CAN HAVE THE PM Cardio AI BOT!! He walked in to triage.
. #1: Emergent Cath Lab Activations with “Normal” Computer ECG Interpretations Spoon Feed A significant minority of code STEMI patients have an initial normal computer ECG interpretation. Consequently, emergency physicians must remain vigilant to identify signs of OMI regardless of the initial computer ECG interpretation.
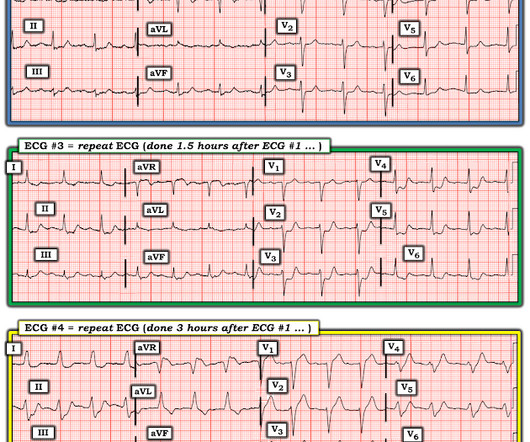
Triage ECG: And here she explains her assessment: The ECG was read as simply "No ST elevation." No repeat ECG was done at this time. Repeat ECG shows no changes." Here is that repeat ECG below, around 3 hours after triage: Repeat troponin during delay rose to 18,700 ng/L. Which is true. None further were ordered.
mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave). The ECG must always be interpreted in clinical context.
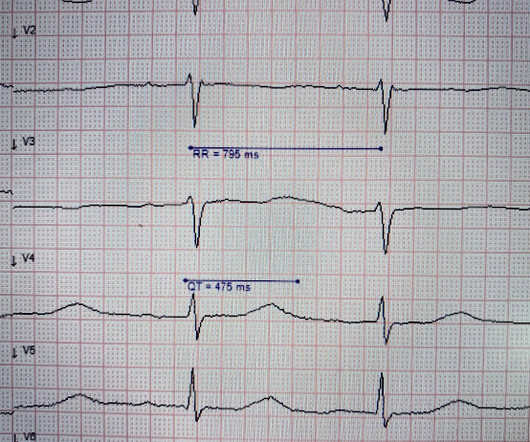
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). A repeat ECG was performed 2 hours after arrival: QTc prolongation ato 722 ms now with alternating T wave pattern (T wave alternans) I texted this to Smith who responded: “T wave alternans and long QT. 2005.08.066.
The ECG below was recorded by EMS. ECG #1 Interpretation: ECG #1 shows sinus rhythm at a heart rate of 77 bpm. At first glance, the ECG does not look too abnormal. In my experience, the pathologic finding in the above ECG is the easiest one to overlook — especially if you are in a rush and do not do a systematic review.
Initial ED ECG: What do you think? Then we must consider clinical data other than the ECG, for a pretest probability : Of all wide complex tachydysrhythmias, the majority are VT. Pretest probability: Even before the ECG, a patient with a history of coronary stent has a 90% chance that his wide complex tachycardia is VT.
The following ECG was obtained. Note that the machine read is "normal sinus rhythm, normal ECG." ECG 1 What do you think? I sent this ECG to Dr. Smith and Dr. Meyers with no clinical context. Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. <0.049 ng/mL).
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. In a patient with syncope and fever, this ECG looks more like Brugada. Smith comment: the ECG in question could be due to Brugada, even though there is a change from baseline. PM Cardio digitized version.
The baseline ECG is basically normal with no ischemia. Here is what the Queen of Hearts says about the Baseline ECG: Active chest pain triage ECG also read as not OMI: She says "not OMI", but she does not have access to the baseline ECG. In the future, we will be able to have her compare with previous and serial ECGs.
The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. How do you interpret the below ECG?
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Provide detailed documentation of the initial assessment, treatment provided, and the patient’s response to interventions. Updated 2023 Jul 17]. Updated 2023 Jul 17]. Chemical Burns. In: StatPearls [Internet]. PMID: 7077702.
Here’s the EMS ECG, digitized with PM cardio. They arrived in the ED 30 minutes later to meet the cardiology team, where an ECG was repeated: Again no STEMI criteria, and there has been improvement in the deWinter and swirl pattern. What do you think? There’s sinus arrhythmia with normal conduction, normal axis and normal voltages.
I was reading EKGs on the system and came across this one: What do you think? No followup EKG was recorded!! See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life.
Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)?
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. See 2 dozen examples here: Understanding this pathognomonic ECG would have greatly benefitted the patient. And ECGs can change and evolve even when there is no ischemia. KEY ECG Features: As per Dr.
Below is the old ECG (on top) and then new ECG (on bottom). The old ECG has proportional ST elevation and T waves. But the new ECG has new Q waves in aVL and V2 (the distribution of the first diagonal artery) – and in the next context of Q waves, the T wave in V2 is upright and relative large. What do you think?
Triage ECG: What do you think? Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Queen of Hearts interpretation: The cardiologist initially was not convinced, stating the ECG was not diagnostic or could not be diagnostic because it was paced.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardial infarction, probably old." I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." Every note says "no ischemic changes on ECG." Deemed "NSTEMI."
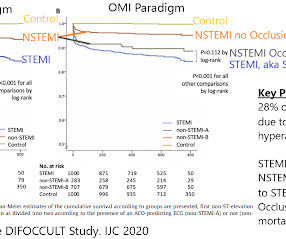
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach. P.S.: Our September 3, 2020 post features Dr. Meyers' 17-minute summary of the OMI Manifesto.
Below is the old ECG, showing that all these changes are new – including the Q waves. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
This ECG was texted to me in real time, but I did not notice the message until about an hour after it came. "50 This was my response: "This looks like a worrisome EKG. But by now you must have a repeat ECG. But by now you must have a repeat ECG. Another ECG was recorded while waiting for the cath team (it was nighttime).
(photocopy of prehospital ECGs digitized by PMcardio) ECG #1 (top): there’s normal sinus rhythm, normal conduction, normal axis, normal R wave progression, and normal voltages. ECG # 2 (bottom): there’s sinus rhythm with normal conduction, normal axis, loss of R wave in V2, normal voltages. Will be missed easily.”
A traditional, left-sided EKG was initially obtained, which demonstrated inverted P waves in lead I, deep Q waves in lead V1, negative QRS complex in V1, and RBBB. It was immediately discerned that the patient had dextrocardia from previous records, and an EKG for dextrocardia was obtained. Figure 1: EKG for Dextrocardia showing STEMI.
Patients confirmed on ECG to have atrial fibrillation or atrial flutter Patients with HR >120 bpm. Pregnant or incarcerated patients Documentation for systolic BP is incomplete Intervention: Administration of IV calcium within 60 min prior to or 30 min after IV diltiazem administration in patients with AF/AFL with RVR.
The triage ECG was sent to me with no history (I did not have access to baseline ECGs), and I said that I thought this was just LVH causing the anterior STE and T waves. I sent this ECG (with no history, no baseline ECG) to Dr. Smith twice, months apart, and he also said LVH without clear OMI. hour delay in this case.
Knowing the capabilities of your system BEFORE disaster strikes is crucial top 10 air care cases of 2023-2024 with drs. If you or your patient do not have a watch capable of providing you with an ECG, consider asking those on board to allow you to borrow theirs. Some newer AED's have the capability of providing you with a rhythm strip.
Here is the result: Next, it interprets the digital data: A perfect interpretation Unfortunately, this ECG was not interpreted as OMI and the patient did not get another ECG recorded until 2 hours later. I tell them that it is not the ECG that is nonspecific, but the interpreter who is nonspecific.
He had a prehospital ECG that was worrisome to the medics, so they called me to see him at the door. His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. and had dilated pupils. He was alert and oriented.
Date: February 1, 2023 Reference: Wolfrum et al. Date: February 1, 2023 Reference: Wolfrum et al. You are tidying your things in anticipation of the arrival of the dayshift when a code blue is called. A post-arrest ECG doesn’t show any signs of STEMI. Circulation. Circulation. The patient is still unconscious.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content