This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiac arrest. How would YOU interpret her post-resuscitation ECG? Does this ECG in Figure-1 provide clue(s) to the etiology of this patient's cardiac arrest? QUESTIONS: In light of the above clinical history.
What do you think of the ECG, and does it matter? I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. 2] This is because, contrary to Bayesian reasoning, the STEMI paradigm is named after and defined by one part of one test: ST elevation on ECG. But only 6.4%
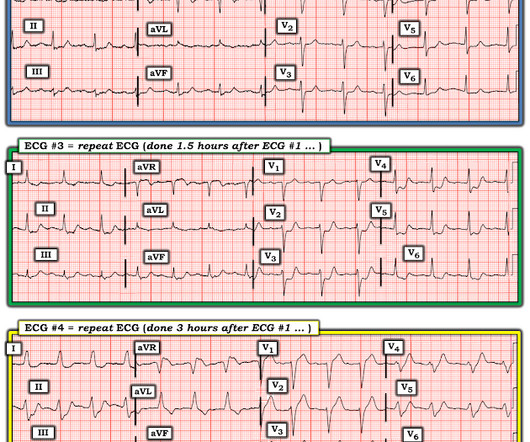
The first EKG is from 2:30 PM on the day of presentation to the ER. My eyes would bulge within a second of viewing this ECG. I texted this to our group "EKG Nerdz," asking "Do you think that anyone could miss this?" No repeat ECG was recorded. The EKG was not repeated until 7 AM the next morning, about 16 hours later.
All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes.
I have often written about how an ECG interpreted as "normal" by a conventional algorithm may well be manifesting OMI, or even long QT or hyperkalemia. Shifa Karim and Gabe Keller helped with a project to assess all these ECGs with the Queen of Hearts. The ECG told the story. I wanted to show some of the cases here.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chest pain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. see reference below) Whats the gold standard for ECG interpretation: is it cardiologist interpretation? What do you think? The latest is Langlois-Carbonneau et al.
Willy is a cardiology fellow with a keen interest in the ECG in OMI. Triage documented a complaint of left shoulder pain. If an immediate EKG was obtained, it was not saved in the medical record. A patient with OMI can have a totally normal ECG!" Cardiology was consulted, and repeat EKG was obtained at around 2:30 AM.
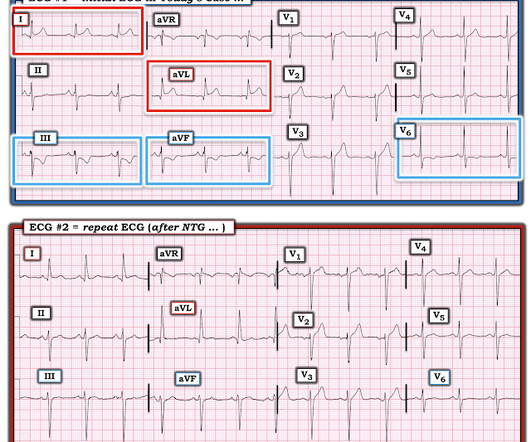
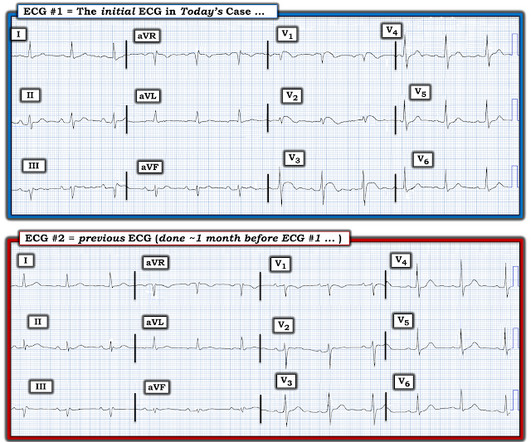
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He had a previous ECG on file: Proving the findings are new The cath lab was activated. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. No other symptoms.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. 1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. But are there any other signs of Occlusion MI?
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). A repeat ECG was performed 2 hours after arrival: QTc prolongation ato 722 ms now with alternating T wave pattern (T wave alternans) I texted this to Smith who responded: “T wave alternans and long QT. 2005.08.066.
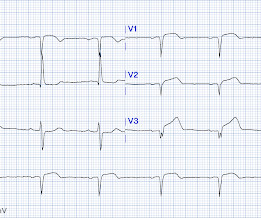
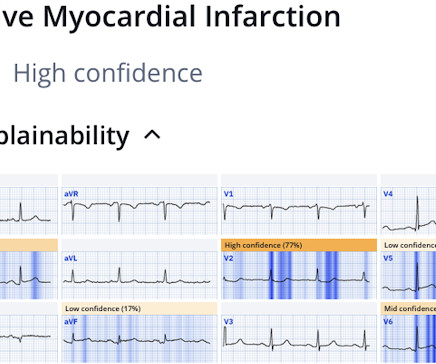
Here was his triage ECG: What do you think? I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2.
EKG, labs, and a CXR are interpreted by the EP as normal. An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. It wasn’t, so you weren’t called, nor did the doc need to document anything. This patient’s history was either poorly taken or poorly documented.
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
The following ECG was obtained. Note that the machine read is "normal sinus rhythm, normal ECG." ECG 1 What do you think? I sent this ECG to Dr. Smith and Dr. Meyers with no clinical context. Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. <0.049 ng/mL).
Initial ED ECG: What do you think? Then we must consider clinical data other than the ECG, for a pretest probability : Of all wide complex tachydysrhythmias, the majority are VT. Pretest probability: Even before the ECG, a patient with a history of coronary stent has a 90% chance that his wide complex tachycardia is VT.
This maneuver improves oxygenation and gas exchange via three main mechanisms (Malhotra, 2022): 1. It is the distending force of the lungs, opposing the innate inward elastic recoil of the lung parenchyma (Neupane and Jamil, 2022). Remove ECG leads and patches. What are the physiologic effects of proning? Suction as needed.
This is her first ECG in the ED: What do you see? This ECG shows both a right bundle branch block and a posterior fascicular block. Another ECG is taken about twenty minutes later and shows this: The rhythm is complex and variable, but overall shows various degrees of AV block. By the end of the ECG, there is 1:1 conduction.
The ECG below was recorded by EMS. ECG #1 Interpretation: ECG #1 shows sinus rhythm at a heart rate of 77 bpm. At first glance, the ECG does not look too abnormal. In my experience, the pathologic finding in the above ECG is the easiest one to overlook — especially if you are in a rush and do not do a systematic review.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. In a patient with syncope and fever, this ECG looks more like Brugada. Smith comment: the ECG in question could be due to Brugada, even though there is a change from baseline. PM Cardio digitized version.
The below ECG was recorded. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. This ECG does not have the typical ST-vector of an LAD occlusion. See below for Ken Grauer Comment on the initial ECG: == On arrival, another ECG was recorded: There appears to have been quite a bit of spontaneous reperfusion!
The ECG below was recorded. The ECG was interpreted as showing atrial flutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. How do you interpret the below ECG?
The baseline ECG is basically normal with no ischemia. Here is what the Queen of Hearts says about the Baseline ECG: Active chest pain triage ECG also read as not OMI: She says "not OMI", but she does not have access to the baseline ECG. In the future, we will be able to have her compare with previous and serial ECGs.
Here’s the EMS ECG, digitized with PM cardio. They arrived in the ED 30 minutes later to meet the cardiology team, where an ECG was repeated: Again no STEMI criteria, and there has been improvement in the deWinter and swirl pattern. What do you think? There’s sinus arrhythmia with normal conduction, normal axis and normal voltages.
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Provide detailed documentation of the initial assessment, treatment provided, and the patient’s response to interventions. 2022 Mar 2;83(3):1-12. Epub 2022 Mar 4. Kirkpatrick JJ, Enion DS, Burd DA. Br J Hosp Med (Lond).
Figure 1: Initial EKG The Case: 45-year-old Spanish speaking male with no known past medical history presented to the ED with 2-3 hours of severe back pain and throat pain. What does this EKG suggest? His EKG suggested a posterior MI as well as other signs of ischemia. Unfortunately, this EKG was not recorded in the EMR.
His ECG is shown: What do you think? The history thus far is highly suggestive of OMI, so we must study the ECG very closely to see if we can confirm this. The Queen of Hearts does not care about rhythm analysis, she simply looks at the ECG and decides whether it represents OMI or not.
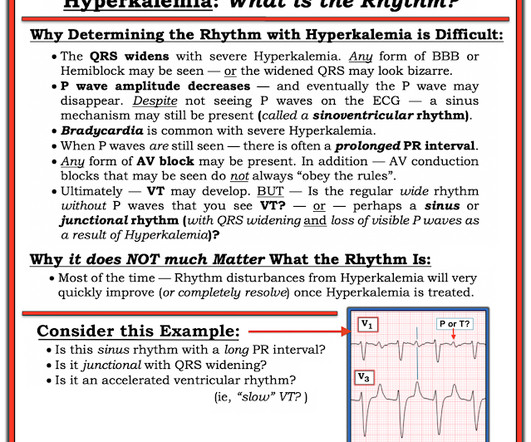
I was reading EKGs on the system and came across this one: What do you think? No followup EKG was recorded!! See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life.
Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)?
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. See 2 dozen examples here: Understanding this pathognomonic ECG would have greatly benefitted the patient. And ECGs can change and evolve even when there is no ischemia. Is this Wellens' pattern A?
This ECG was recorded: The computer called it "Normal" except for "Possible right ventricular conduction delay" What do you think? The team was there and I showed them the ECG and said "I am 80% certain this is OMI. While waiting for the cath team, a 3rd ECG was recorded: Now there is STE in V6, with large T-waves in V4-V6.
Her presenting ECG is shown below: ECG 1 What do you think? I had previously run this ECG through QOH in the PMcardio app environment and she reported mid confidence, shown below. You can see that version 2 has a higher number than version 1, hence she sees the ECG as more OMI-like than version 1. I sent this to Drs.
Triage ECG: What do you think? Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Queen of Hearts interpretation: The cardiologist initially was not convinced, stating the ECG was not diagnostic or could not be diagnostic because it was paced.
Below is the old ECG (on top) and then new ECG (on bottom). The old ECG has proportional ST elevation and T waves. But the new ECG has new Q waves in aVL and V2 (the distribution of the first diagonal artery) – and in the next context of Q waves, the T wave in V2 is upright and relative large. What do you think?
Here are his three EMS ECGs: EMS1 at 0735 This was sent to Dr. Smith with no other information. Meyers sent this ECG to Smith without any other info and this was the response: Smith interpretation: "A very rare anterior OMI w high S-wave voltage." ED ECGs: 0814 0830 These show continued reperfusion with no evidence of reocclusion.
His vitals were normal and his first ECG was as shown below: There is obvious ST segment elevation (STE) in anterior leads. Is this a subtle ECG ? This was a clearly diagnostic ECG that makes me think of a proximal left anterior descending artery (LAD) occlusion. A second ECG was taken at 15:16. Wait for the angiogram.
September 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called www.First10EM.com Case: You are working an overnight shift at a small rural hospital. You are tidying your things in anticipation of the arrival of the dayshift when a code blue is called. Circulation.
3 You order toxicology labs, an EKG, and a sitter to observe. After resuscitation, the patient should be evaluated by a multi-disciplinary team in the hospital to re-affirm the patient’s code status and medical treatment goals. 2022 Jun;34(3):473-474. The initial QTc is normal, but on repeat becomes prolonged. J Med Ethics.
Keyes 2022) Auditory and Visual Hallucinations (AH/VH) : The differential diagnosis for hallucinations is broad and includes medical pathology, psychiatry pathology, and transient causes such as acute drug intoxication. As always, document clinical sobriety before discharge. 2022 Jul;46(7):1306-1312. Alcohol Clin Exp Res.
1,4-5 Thus, an electrocardiogram (ECG) and cardiac monitoring should be performed for unstable, electrical injury patients. 7 Thus, an ECG is recommended for all electrical injuries. His ECG was unremarkable. Documentation with coronary arteriography within 12 1/2 hours of the onset of symptoms in two cases (three episodes).
ICD-10 codes: F00-03 are the ICD codes for dementia and its subtypes F02. It is important to complete an ECG prior to initiating pharmacological therapy as drugs, such as antipsychotics can prolong the QT interval, increasing the risk of arrhythmias. If there is no benefit this should be stopped.
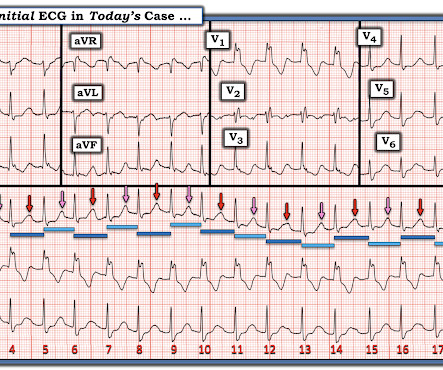
Given her reported chest pain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? This patient was reported to have distant heart sounds but was not hypotensive and did not have JVD according to documentation. For clarity in Figure-1 — I've reproduced her initial ECG.
Now, for selected patients, emergency physicians can leverage low and non-rising high sensitivity troponin values and a low HEART score (composed of history, ECG, age, risk factors, and troponin level) to implement outpatient follow-up plans safely, within a few hours. Updated September 21, 2022. February 22, 2022.
This patient’s syncope is most likely due to metabolic disruptions and fluid-status physiology; nevertheless, assessment of cardiogenic etiologies through an EKG, troponin, and cardiac risk factors should be considered as appropriate. There have been documented cases of overdose, and of note, there is no known antidote.
Patient 1 (ECG on the left) was a 45 year-old male, and patient 2 (ECG is on the right) was a 70 year-old male. Using T wave amplitude, can you tell which ECG has hyperacute T waves? What other parts of the ECG would you like to see, and how will you use this to refine your interpretation?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content