This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Methods We investigated four 18-month periods between 2005 and 2018. Inclusion criteria were non-traumatic cardiac arrests treated with at least one external electric shock with an automated external defibrillator from the basic life support team and resuscitated by a physician-staffed ALS team.
In trauma patients, the primary sources of bleeding are external haemorrhage (blood on the floor), chest, abdomen, pelvis, and long bones in paediatrics brain is also included (infants with open sutures can bleed a significant amount intracranially) Shock The most common cause in trauma is haemorrhage.
1 Though hydrocortisone is often included in ‘crash carts,’ the most recent consensus on cardiopulmonary resuscitation (CPR) has a weak recommendation against the use of corticosteroids during CPR. 6 However, due to the vasoconstrictive effects, hydrocortisone may be useful in refractory shock. October 19, 2018.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. In this case, profound shock for 1 hour would result in the same degree of infarction. The Type 2 MI would then have been a result of the prolonged severe shock while in arrest. After good ECMO flow was established, she was successfully defibrillated.
Survival After Intravenous Versus Intraosseous Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Shock-Refractory Cardiac Arrest. Survival After Intravenous Versus Intraosseous Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Shock-Refractory Cardiac Arrest. Date: August 12th, 2021 Reference: Daya et al.
Date: December 6th , 2018 Reference: Perkins et al. Date: December 6th , 2018 Reference: Perkins et al. You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). He is unsuccessfully shocked. Reference: Perkins et al.
Was the patient thrown from the source (suggestive of DC shock and may result in further blunt force trauma)? Children, especially toddlers, may insert objects into outlets, leading to shocks or burns. Electrical devices used near water sources can cause severe shocks. Was the voltage high or low (as below)?
10 The score predicts the probability of survival to hospital discharge using a number of factors including CPR duration, serum potassium, core temperature, age, and suspected mechanism of hypothermia. 2,11 There are cases of patients recovering after hours of time without a pulse with good CPR. Resuscitation 2018.
JACC Cardiovasc Interv 2018. in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 A Randomized Trial of the Optimum Duration of Acoustic Pulse Thrombolysis Procedure in Acute Intermediate-Reisk Pulmonary Embolism: The OPTALYSE PE Trial. PMID: 30025734 Sharifi M et al. Am J Cardiol 2013. PMID: 23102885 Aykan AC et al.
For anyone approaching a structured ABC would be a priority to establish whether shock was present or not. Typical features include: HR >220bpm Narrow complex regular tachycardia P waves difficult to identify In this case there is no shock present so we can proceed to the right branch of the ALSG guideline.
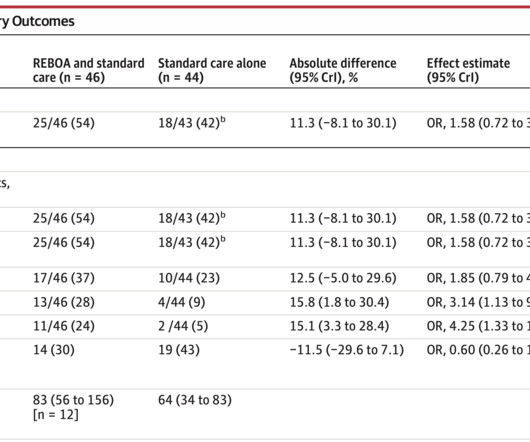
Military practice guidelines recommend REBOA for profound shock (SBP <90mmHg) 1 and ACEP along with the American College of surgeons recommend REBOA for traumatic life-threatening hemorrhage below the diaphragm in patients with hemorrhagic shock who are unresponsive or transiently responsive to resuscitation. J Spec Oper Med.
Thankfully, that gentleman was successfully resuscitated despite no bystander CPR, and if you listen carefully, we hope to arm you with the tools to do so similarly. In total, they pulled references from 1966 until 2018. Nachi: Each year, in the US, approximately 10,000 patients present with electrical burns or shocks.
This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF).
4) This higher likelihood of attaining return of spontaneous circulation (ROSC) is contingent upon high quality CPR and early defibrillation. One therapy is vector change defibrillation, in which the defibrillation pads are placed in the anterior posterior configuration to change the direction of the shock delivered through the myocardium.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. Angiography was technically challenging as the patient was receiving CPR, but the cardiologist suspected acute stent thrombosis and initiated cangrelor, although no repeat angiography was able to be obtained.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content