This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
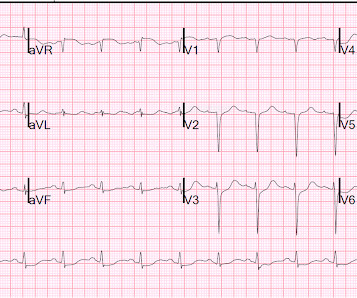
The ECG in Figure-1 was obtained following successful resuscitation. Stat Echo — obtained shortly after successful resuscitation revealed anterior wall akinesis. QUESTIONS: In view of the above history — How would YOU interpret the ECG in Figure-1 ? Is this ECG finding present in today’s initial ECG?
The ECG in Figure-1 was obtained from an elderly woman — who presented to the ED ( E mergency D epartment ) for dyspnea on exertion over recent weeks. Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). What are YOUR "Quick Thoughts" about this case?
Hemodynamic instability and ongoing cardiac arrhythmias are a strong contraindication as chest access for cardiopulmonary resuscitation is limited (Koulouras et. Remove ECG leads and patches. Reattach EKG leads to back. 2013; Mi et. The PROSEVA study is the most recent and famous randomized control trial.
Circulation Assess heart rate, blood pressure, peripheral and central CRT, pulses and 3 lead ECG. Establish IV access and begin fluid resuscitation with 250ml boluses of 0.9% This includes adequate pain control, fluid resuscitation, and stabilization of any systemic complications. 2013 May;74(5):1363-6. doi: 10.1097/TA.0b013e31828b82f5.
ECG: to monitor T wave changes due to hypokalaemia. ECG features of Hypokalaemia: Increased P wave amplitude (peaked P waves) Prolonged PR interval Widespread ST depression T wave flattening or inversion Prominent U waves (most noticeable in the precordial leads) Figure 2 : ECG of a patient with serum K+ of 1.9
It is worth noting, that with “Sepsis 3” many of these terms will become out-of-date – but validation work is required… The Rivers’ paper can be accessed here: [link] It was a single centre study which compared standard care with protocolised resuscitation packaged together as early goal-directed therapy (EGDT).
An immediate 12-lead EKG was obtained: There is ST elevation in leads aVR and V1, with marked ST depression in I, II, III, aVF, V3-V6. In addition, the patient received 750 mL of fluid resuscitation with transient improvement of blood pressure. What should be done? Should the cath lab be activated?
The following 12-lead ECG was recorded at 11 minutes after ROSC. at the time of the ECG. Here is the annotated ECG from above, with lines drawn. Here is an article I wrote: Updates on the ECG in ACS. The patient was resuscitated for 50 minutes, and then this ECG was recorded: Sinus rhythm. Mg was 1.6.
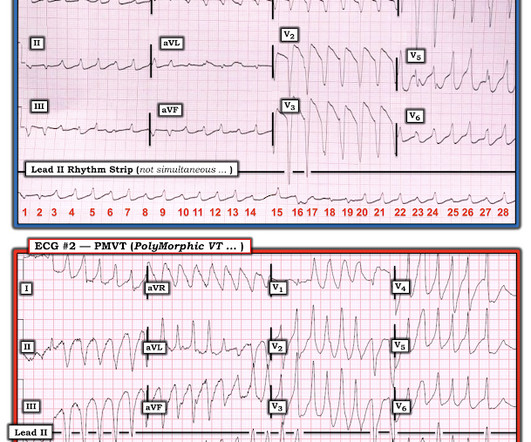
== MY Comment by K EN G RAUER, MD ( 6/1 /2020 ): == YOU are asked to interpret the ECG shown in Figure-1. Figure-1: The initial ECG in the ED. MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ).
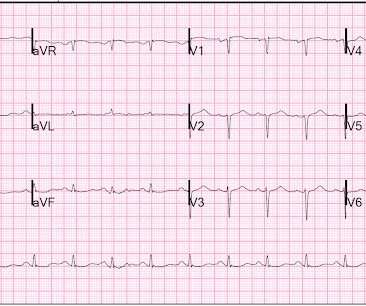
What is your ECG interpretation and what would you do next? This ECG shows a normal sinus rhythm with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, late R wave progression (and misplaced V2), normal voltages, ST-elevation in aVR and global ST-depressions. BP was 110 and oxygen saturation was normal.
Given her reported chest pain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? 2013 Sep;26(9):965-1012.e15. The beat-to-beat variation in the QRS complexes (electrical alternans) is a classic ECG finding of a large pericardial effusion or pericardial tamponade. J Am Soc Echocardiogr.
Jeff: Do note, however that 2013 guidelines do not recommend one procedure over another and leave that decision up to local surgical expertise, patient specific risk factors, and treatment goals. Nachi: Check an EKG immediately after arrival for any patient that may be concerning for ACS. Obesity (Silver Spring).
When I was an inpatient pharmacy manager in 2013, my hospital was visited by the California Department of Public Health (CDPH), concerned about droperidol and ECG monitoring, or rather, lack thereof. Fast forward to now, and it seems droperidol is still a favorite punching bag for CDPH. Guideline directed!) The realistic (or preferred?)
Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. This ECG is diagnostic of diffuse subendocardial ischemia. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI.
Some total LAD occlusion manifest on the ECG similarly to some left main occlusions. Depending on where the STE vector of the LM occlusion shows up on the ECG, there may be either STE, or STD, or neither in aVR, and lead aVR will not be the important part of the ECG interpretation in these cases.
Electrocardiography (ECG) should be performed on any patient with significant blunt chest injury. A negative ECG is highly consistent with no significant blunt myocardial injury. Any patient with a new abnormality on ECG (dysrhythmia, heart block, or signs of ischemia) should be admitted for continuous ECG monitoring.
Audrey’s academic interests include trauma and resuscitation. Audrey’s academic interests include trauma and resuscitation. The first visit was back in 2013 for SGEM#50 : Under Pressure – Vasopressin, Steroids and Epinephrine in Cardiac Arrest. Robert’s academic interests include research and evidence-based medicine.
Fluid resuscitation was initiated. Here is the initial ED ECG: What do you think? The ECG shows peaked T waves, QRS widening, a coved-type ST segment with inverted T waves most prominent in V1 and V2 consistent with Brugada pattern. They opined that the ECG could instead be "metabolic." Creatinine elevated at 3.09
As resuscitation measures are underway, you obtain collateral from EMS and parents. If a wide complex rhythm is present on ECG, sodium bicarbonate boluses (to overcome sodium channel blockade) should be administered. 2013 Jan;33(1):38-43. The Case: A 4-year-old boy born with no past medical history presents in cardiac arrest.
Key Concepts Quickly rule out life-threatening emergencies that require immediate resuscitation. rebound tenderness), getting an EKG if you have a high suspicion for cardiac involvement, or using ultrasound to assess for free fluid. Think aortic aneurysm dissection, bowel perforation, STEMI (especially in elderly female patients!),
Whilst we’ve ‘re-discovered’ balanced resuscitation (first described by Cannon back after WWI), there remains some limited controversy – listen to this 2013 take from Simon Carley at St. An ideal resuscitation would allow parallel processing with a designated team leader and teams devoted to various tasks.
This was her prehospital ECG: What do you think? ECG many months later: RBBB with well-formed Q-waves in V1-V6, also I, aVL. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiac arrest resuscitation. For clarity in Figure-1 I've reproduced and labeled this initial ED ECG.
She was resuscitated and admitted to ICU for presumed sepsis. Hint: What does the arterial waveform correspond to on the ECG? And you can see a sharp deflection in the ECG from pacing artifact. adapted from Grauer K: ACLS-2013-ePub Section 15, KG/EKG Press ). Her family had not heard from her and called EMS.
Below is his presentation ECG. The above ECG was originally recorded with a paper speed of 50mm/sec. Interpretation: The ECG shows sinus rhythm at 94 beats per minute. This ECG shows a lot of "acuity". The ECG findings in isolation must be assumed to be acute MI until proven otherwise. What do you think?
Her first ECG is shown. After this ECG was obtained, the ER physician received word that the patient's husband had died in the crash. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Overall bland.
Initial echocardiogram (ECG) on arrival (see figure 2) to our emergency department revealed normal sinus rhythm, mild interventricular conduction delay (RSR’), and possible right ventricular hypertrophy. This ECG in combination with presenting symptom of cardiac arrest raised suspicion for Brugada syndrome. Figure 2: The initial ECG.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content