
Case Report: The Not So Normal, Normal EKG
ACEP Now
AUGUST 12, 2024
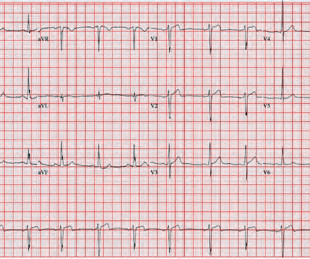
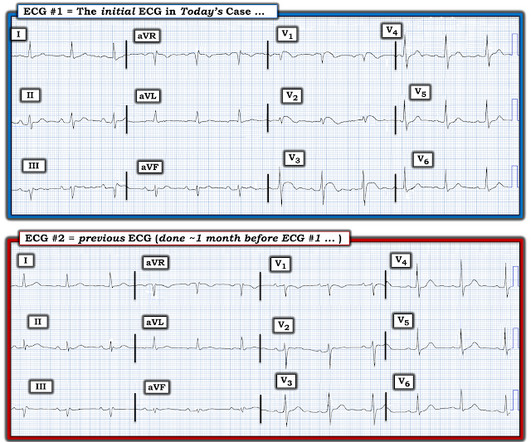
The patient had an EKG performed within 10 minutes of arrival while in triage (see Figure 1). In the absence of significant ST elevations, the EKG was signed and the patient was placed back in the queue to await a bed. FIGURE 1: First ED EKG. Given his EKG findings and presentation, he was started on heparin and admitted.
































Let's personalize your content