This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
pdf Equipment required for resuscitative thoracotomy: Surface anatomy: Appearance of pericardial clot A foley catheter being used to fill a cardiac wound – note how easily this could be pulled out. An open chest with aortic compression Simulation of resuscitative thoracotomy by London HEMS team. EMJ; 2005: 22-24.
It might be better to consider traumatic cardiac arrest as a completely different disease eg LOST: Low Output State due to Trauma The 2015 European Resuscitation Council and UK Resuscitation Council Algorithms for Traumatic Cardiac Arrest: To read the whole ERC guideline on special circumstances cardiac arrest including trauma, click here.
Finally, anticipating and addressing known complications such as seizures, increased intracranial pressure, or cerebral edema with appropriate measures, including antiepileptic drugs or osmotic agents, is essential for improving patient outcomes. Lowering the MAP may mitigate these risks and possibly improve outcomes. doi: 10.1161/01.str.0000014509.11540.66.
This episode of PEM Currents discusses ECPR (Extracorporeal Cardiopulmonary Resuscitation), an advanced procedure used in cases of cardiac arrest when traditional CPR fails. Extracorporeal Cardiopulmonary Resuscitation. 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care.
Background Therapeutic hypothermia, later rebranded as targeted temperature management, became a standard post-cardiac arrest therapy for comatose patients after two 2002 NEJM trials ( n=273 and n=77 ) suggested reducing core temperature to 32°C to 34°C markedly improved neurologic outcomes and survival.
Targeted temperature management (TTM) for patients following cardiac arrest resuscitation has gone through several dosing iterations in the past two decades. Finally, the guidelines support active temperature management’s (though not necessarily hypothermia) role in improving post-arrest outcomes. degrees Celsius for 72 hours.
Does Functional Outcome Improve with Time Postsurgery for Hirschsprung Disease? J Pediatr 2005; 146:787. J Pediatr Surg 2005; 40:197. Single-stage versus multi-stage pull-through for Hirschsprung's disease: practice trends and outcomes in infants. Hirschsprung disease, associated syndromes and genetics: a review.
Background Therapeutic hypothermia, later rebranded as targeted temperature management, became a standard post-cardiac arrest therapy for comatose patients after two 2002 NEJM trials ( n=273 and n=77 ) suggested reducing core temperature to 32°C to 34°C markedly improved neurologic outcomes and survival.
This has been the central question of many research projects with variable outcomes. One such study of 263 patients without hypertensive emergencies treated in a resuscitation unit found that 40% of patients had a MAP difference ≥ 10 mmHg between IABP and NIBP measurements. Crit Care Med 2005; 33: 1276 –1280 6. Gelmann, D.,
7 Workup other than serum iron concentration at 4 hours after ingestion not shown to accurately predict clinical outcomes or severity of toxicity. Aggressive fluid resuscitation as patients may be severely hypovolemic from GI symptoms. Case Follow-up: The patient received a fluid resuscitation with 20 mL/kg bolus of normal saline.
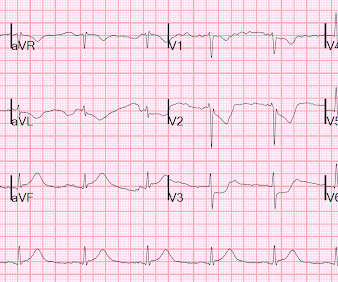
He could not be resuscitated. To quote Dr. Stephen Smith: "The worst risk factor for a bad outcome in acute MI is young age." Unfortunately — the cardiologist at that center did not recognize the abnormal ECG findings. The patient was discharged without repeating the ECG. The patient arrested outside the hospital.
The exact mechanism is not known… It was previously believed that it was due to rapid changes in serum osmolality during initial fluid resuscitation. 2005 May;146(5):688-92. Factors associated with adverse outcomes in children with diabetic ketoacidosis-related cerebral edema. The mortality rate for cerebral edema is 21%–24%.
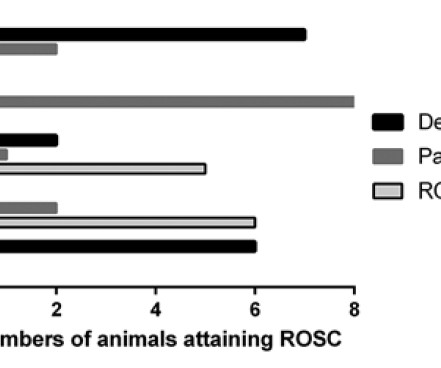
Methods We investigated four 18-month periods between 2005 and 2018. The first period was considered baseline and included patients from the randomised controlled trial ‘DEFI 2005’ The three following periods were based on the Paris Sudden Death Expertise Center Registry (France).
Eur J Haematol 2005; 75:1. Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Time to antibiotics and outcomes in cancer patients with febrile neutropenia. September 30, 2005. Give appropriate fluids, vasopressors, and antibiotics.
Evaporative cooling is the preferred method to actively reduce body temperature in the emergency department , as it can be performed with ongoing resuscitation efforts. Ice water immersion and iced peritoneal lavage are additional methods used to lower temperature but are more invasive or can prevent additional resuscitative efforts.
After resuscitation, he was found to have a 90% thrombotic lesion in the same saphenous vein graft to the right posterior descending artery. The patient stabilized and had a good outcome. I saw this 30 year old woman with no cardiac disease who was resuscitated from ventricular fibrillation : Classic Hypokalemia, with large U-waves.
Nevertheless, mortality of prehospital traumatic cardiac arrest (TCA), and survivability with good neurologic outcome, remain the gold standards of trauma care in and out of the hospital and are effectively the criterion by which we measure outcomes in the trauma literature. Discussion: Dead On Scene: The 96.2% mortality rate and 43.5%
Qvigstad et al showed in again in Resuscitation in 2013, confirming inter-individual variation in effectiveness of CPR using ETCO2 as a surrogate for CO Trauma Deakin et al. (J. trauma 2004) showed that end-tidal CO2 may be of value in predicting outcome from major trauma (19). O Capnogram showing rebreathing during inspiration.
Trauma surgeons have traditionally relied on ABGs to assess acid-base status for overall prognostication of trauma injury severity and to screen for occult injury or malperfusion, as this might alter management and aggressive resuscitation. As previously noted, ABGs are not easily obtained (let alone in the critically ill trauma patient).
In other patients who are stable and the bleeding has resolved, CTA is of low yield If they are critically ill and have severe bleeding, resuscitate first and consult IR, radiology, and surgery. There is no clear improvement with idarizucimab or andexanet alfa on patient-oriented outcomes. 2005 Jun 1;21(11):1281-98.
With opportunities to improve outcomes for both the fetus and the mother, I’m confident that this episode will be worth your time. Nachi: For patient who have a threatened miscarriage in the first trimester, there is a 2-fold increased risk of subsequent maternal and fetal adverse outcomes.
Sepsis There has been much controversy over the last two decades around the various nuances of volume resuscitation in ED patients with suspected sepsis, much of which goes beyond the scope of this limited review. In lower-resource settings, the evidence is stronger against a liberal approach to volume resuscitation. Andrews et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content