This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
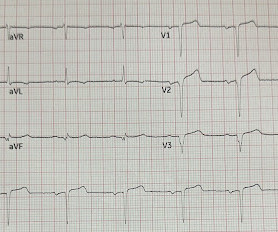
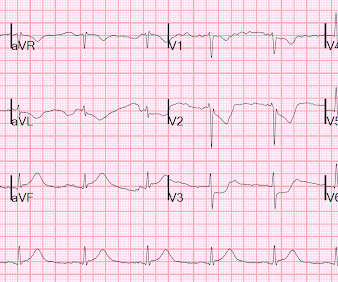
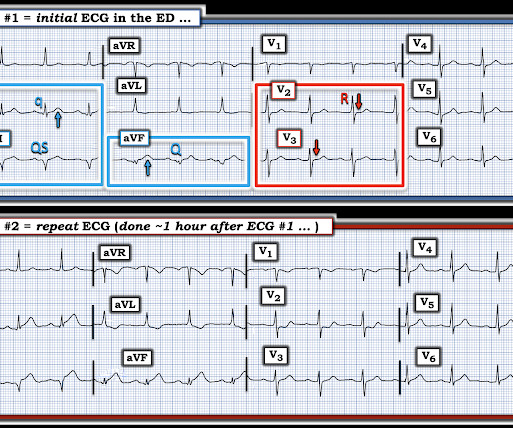
The ECG in Figure-1 was obtained from a previously healthy man in his early 20s — who initially presented with GI symptoms, that then evolved into CP ( C hest P ain ). QUESTIONS: Given the above history — How would YOU interpret the initial ECG that is shown in Figure-1 ? Figure-1: The initial ECG in today's case. (
EKG Reasonable screen for cardiac etiology [ Kane, 2010 ]: Chest Pain with Exertion? 2005 Jun;33(6):1231-8. Is there a family history of sudden death, hypertrophic cardiomyopathy, long QT syndrome, or tachyarrhythmias? Chest Pain in Children: A Reasonable Work-up The goal is to balance risk of the rare with risk of over-testing.
Here is the ED ECG (a photo of the paper printout) What do you think? American Journal of Emergency Medicine 2005; 23(3):279-287. The "good news" — is that a cardiac-related cause of syncope is unlikely if the initial ECG is normal, and cardiac monitoring in the ED fails to reveal significant arrhythmia.
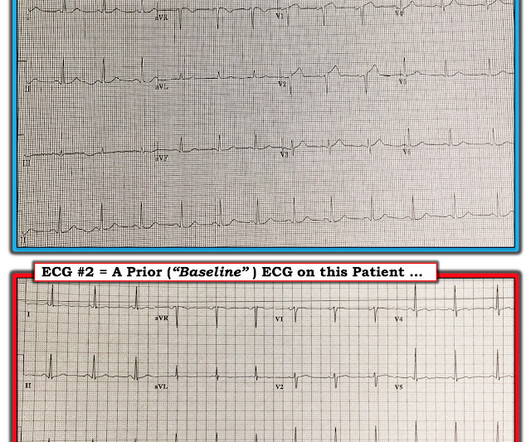
These diagnoses were not found in his medical records nor even a baseline ECG. An ECG was obtained shortly after arrival: What do you think? There is no evidence of WPW on this ECG, but it is diagnostic for OMI. If the LAD is completely occluded, then why does the ECG show reperfusion? What are we seeing here?
Here is the ECG: Sinus tachycardia. This is an extremely dangerous ECG. When the ECG shows the effects of hypokalemia, it is particularly dangerous. Here are the American Heart Association Guidelines: 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Part 10.1:
What are the worrisome EKG findings, and what is the differential diagnosis? If you want a rule, I derived one a few years ago (AJEM 23(3):279-287; May 2005). I cannot tell from this ECG if it is 12 hours or 12 years since the MI. 70 yo with h/o MI, recent CABG, has acute onset of chest pain. What is the most likely diagnosis?
A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy? What does a heart look like on ultrasound when the EKG looks like that? The followup ECG is here: Now the QRS is only slightly prolonged. A middle-aged woman was found down in her apartment unconscious. She was in shock with thready pulses.
This ECG was recorded on arrival: What do you think? Proof that all STE and hyperacute T-waves in the presentation ECG are new. They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG shows persistent Occlusion MI but does not meet STEMI criteria.
What do you think of this ECG in a patient with chest pain? An ECG was obtained at triage: ECG #1 at 0000 hours. The ST depression in V6, and T wave flattening/inversion in V6 and aVL, also support LVH The ECG was repeated to get a clearer tracing and because her pain increased to 10/10 at that moment.
Meyers ECG Interpretation: Easily diagnostic of LAD occlusion. The ECG easily meets STEMI criteria in all leads V2-V6, as well. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chest pain. The ECG was interpreted as "benign early repolarization." This gets drilled into them.
The only statistically significant factor intra-arrest was the first ECG rhythm, which only had an odds ratio of 1.12, which is relatively low. Many studies suggest that increased time spent on scene correlates with worse outcomes for trauma (Stiell 2008) and all-cause incidence (Isenberg 2005) across all levels of prehospital care.
Here is his ED ECG: There is obvious infero-posterior STEMI. This subsequent ECG was recorded after the K was up to 2.2 The QT is much shorter There are now clear U-waves in V2 and V3 2 days later, this ECG was recorded with a K of 3.5: These two rhythms are often indistinguishable on the monitor or ECG. This was stented.
Electrocardiography (ECG) should be performed on any patient with significant blunt chest injury. A negative ECG is highly consistent with no significant blunt myocardial injury. Any patient with a new abnormality on ECG (dysrhythmia, heart block, or signs of ischemia) should be admitted for continuous ECG monitoring.
Abnormal ECG – looks for cardiac syncope. Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. If no previous ECG was available, ECG was classified as abnormal if any abnormality was present. orthostatic vitals b.
A 12-lead EKG shows sinus tachycardia but is otherwise normal. 2005 Oct 5;9(5):R498-501. Triage vital signs include BP 80/40 mm Hg, HR 154 bpm, T 41C rectal, RR 28 breaths per minute, saturation 94% on room air. The patient is agitated, not oriented, and becoming combative with ED staff. Temps greater than 41.5C doi: 10.1186/cc3771.
Pain can be associated with a friction rub on cardiac auscultation, a pericardial effusion on a bedside echocardiogram, or diffuse ST elevations on an EKG. 2005 Jul-Aug 2005;12(4):311-9. Up to two-thirds of rib fractures are missed on initial chest radiographs. Jan 23 2008;(1):CD000396. doi:10.1002/14651858.CD000396.pub3
EMS arrived and recorded this ECG: What do you think? Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. Inferior and posterior OMI without STEMI criteria.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content