This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This article will explore the ten essential features of the Defibtech DBP 2003 AED Battery, a cutting-edge power source designed to provide optimal performance and peace of mind. Long-lasting Durability The Defibtech DBP 2003 AED Battery is built to last, offering exceptional durability that ensures longevity.
Among the wide range of defibrillators available on the market, the Defibtech DBP 2003 stands out as the ultimate choice for emergency response teams. With its advanced features, user-friendly design, and exceptional performance, the DBP 2003 is a game-changer in emergency medical care.
2003 Jul;40(7):620-5. Pediatric adjusted reverse shock index multiplied by Glasgow Coma Scale as a prospective predictor for mortality in pediatric trauma. Systematic review showed 85% of studies with substantial reliability with kappa statistic >0.6 Fun fact for animal lovers!- Indian J Pediatr. 2001 Apr;68(4):311-4. Biradar, S.
2 This requirement was ultimately removed in 2003, however iron related exposures and deaths have stayed low. Stage 3 (timing variable) Shock 1 : Can occur within hours for massive ingestion, but may occur over a longer time course. This stage does not always occur. This stage is not truly quiescent as cellular toxicity progresses.
Penn-Barwell JG, Roberts SA, Midwinter MJ, Bishop JR: Improved survival in UK combat casualties from Iraq and Afghanistan: 2003-2012. In patients with penetrating trauma permissive hypotension may remain useful for longer or at least until a patient can be differentiated and the bleeding controlled. Lots to think about! 2016 Jul;46(1):3–16.
Pediatr Surg Int 2003; 19:439. Pediatr Surg Int 2003; 19:247. 2003; 12(4):241-253. 2003; 21:909-935. Khan AR, Vujanic GM, Huddart S. The constipated child: how likely is Hirschsprung's disease? Singh SJ, Croaker GD, Manglick P, et al. Hirschsprung's disease: the Australian Paediatric Surveillance Unit's experience.
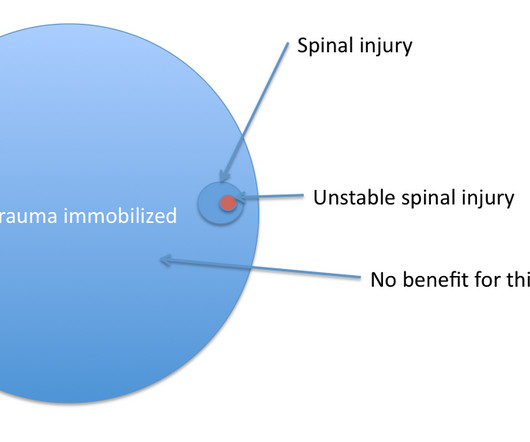
2003 Dec 25;349(26):2510–8. Journal of Emergencies, Trauma, and Shock. References Stiell IG, Clement CM, McKnight RD, Brison R, Schull MJ, Rowe BH, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. Oteir AO, Smith K, Stoelwinder JU, Middleton J, Jennings PA. A systematic review.
2003 Jun;111(12):1805-12. 2003 Jul;112(2):299. 2003 Jun;111(12):1805-12. 2003 Jul;112(2):299. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Serological reactions in pneumonia with non-protein somatic fraction of pneumococcus. J Clin Invest. C Reactive Protein.
Authors' commentary: Cardiogenic shock in the setting of severe aortic stenosis. This patient’s severe aortic stenosis (AS) and associated severe cardiogenic shock likely created the ECG pattern, resulting in a very difficult challenge for our inpatient team. Fundamentally, cardiogenic shock is an issue of decreased cardiac output.
You can also see when your treatment is working- if you give a patient in septic shock some fluid and improve their CO, you’ll see a rise in ETC02 You can confirm adequacy of respiratory function in the fitting or post-ictal patient when all other methods fail PITFALLS Device failure- lines blocking, batteries running out, pump failure.
We designed a step-up protocol in which shocks at 50, 100, 200, 300, and 360 J were used for transthoracic cardioversion. Ballatore et al — Medicina (Kaunas) 55(8): 497, 2019 — and — Page et al — Circulation 107:1141-1145, 2003 ). An estimated 10-to-40% of all patients with AFib do not have symptoms associated with this arrhythmia.
He is in compensated shock. Clin Chest Med 24 (2003) 473– 487 The Huber needle is not a resuscitative line. Obtain proper access to give fluids -- do not rely on the port-a-cath. Vascular devices are notoriously troublesome. In the European Respiratory Journal, Munck et al. Pediatr Nurs Nov 2005 Vol 31, No 6 Trachsel D, Hammer J.
The infant in shock after a ‘cold’: myocarditis Beware of the poor feeding, tachycardic, ill appearing infant who “has a cold” because everyone else around him has a ‘cold’. 2003; 18(2):150-151. That may very well be true, but any virus can be invasive with myocardial involvement. DOI: 10.5772/56177. Toxins De Chadarévian JP et al.
First, there can be a poor correlation between venous and arterial gases in states of shock, hemodynamic instability, or extremes of acid-base disturbances, due to poor cardiac output/circulatory failure impairing venous and arterial flow, with associated poor gas exchange as well as hypercapnia and acidemia at the tissue level (8).
However, it must be considered in toxic-appearing patients, those with prosthetic heart valves, artificial joints, or immunocompromised states Clinicians must keep a broad differential and consider other conditions such as necrotizing fasciitis, clostridial myonecrosis, compartment syndrome, toxic shock syndrome, etc. pneumoniae , S.
Children have long suffered from an under-treatment of their pain, due both to our incomplete acknowledgement of their pain and our fear of treatment ( Howard 2003 ). Unexplained tachycardia may be the early signs of shock. 2003 Nov 12;290(18):2464-9. 2003 Jan;90(1):5-9. Horeczko T, Mahmoud MA. Curr Opin Anaesthesiol.
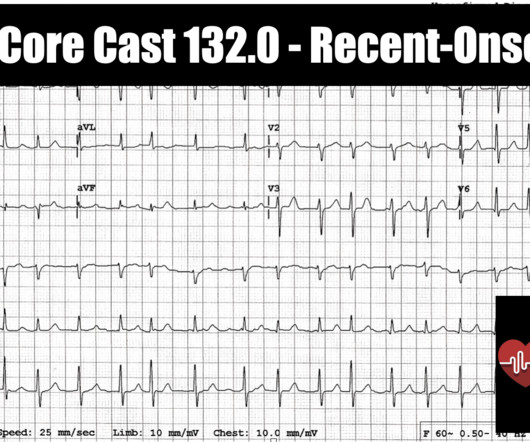
PMID: 25701296 The SGEM: Shock Through the Heart (Ottawa Aggressive Atrial Fibrillation Protocol) ALiEM: Atrial Fibrillation Rate Control in the ED: Calcium Channel Blockers or Beta Blockers. JACC 2003; 41: 255-62. REBEL Core Cast 132.0 – Recent-Onset AFib Click here for Direct Download of the Podcast.
Symptoms may be non-specific in the beginning with patients quickly developing septic shock and disseminated intravascular coagulation. 2003; 5: 229–240. Patients with asplenia are at risk of infections by encapsulated organisms: Streptococcus pneumoniae , Haemophilus influenzae , Neisseria meningitidis and other bacteria such E.
Sheridan (2003). Triple antibiotic coverage is recommended. Suggested regimens include: Ampicillin AND Gentamicin AND Clindamycin OR Metronidazole Update tetanus vaccination Usually requires dilation and curettage to remove any retained products of conception or foreign bodies. References: Abbrescia, K. PMID: 12962354 Apantaku, O.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content